

High platelet count as a link between renal cachexia and cardiovascular mortality in end-stage renal disease patients
- PMID: 21813809
- PMCID: PMC3155928
- DOI: 10.3945/ajcn.111.014639
High platelet count as a link between renal cachexia and cardiovascular mortality in end-stage renal disease patients
Abstract
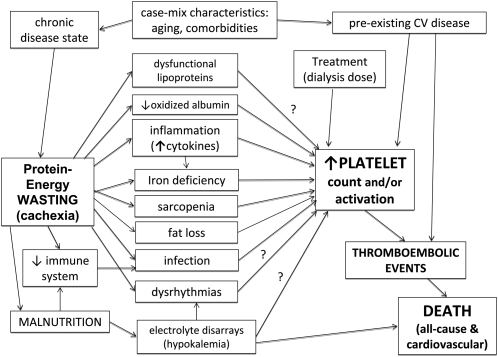
Background: It is not clear why cardiac or renal cachexia in chronic diseases is associated with poor cardiovascular outcomes. Platelet reactivity predisposes to thromboembolic events in the setting of atherosclerotic cardiovascular disease, which is often present in patients with end-stage renal disease (ESRD).
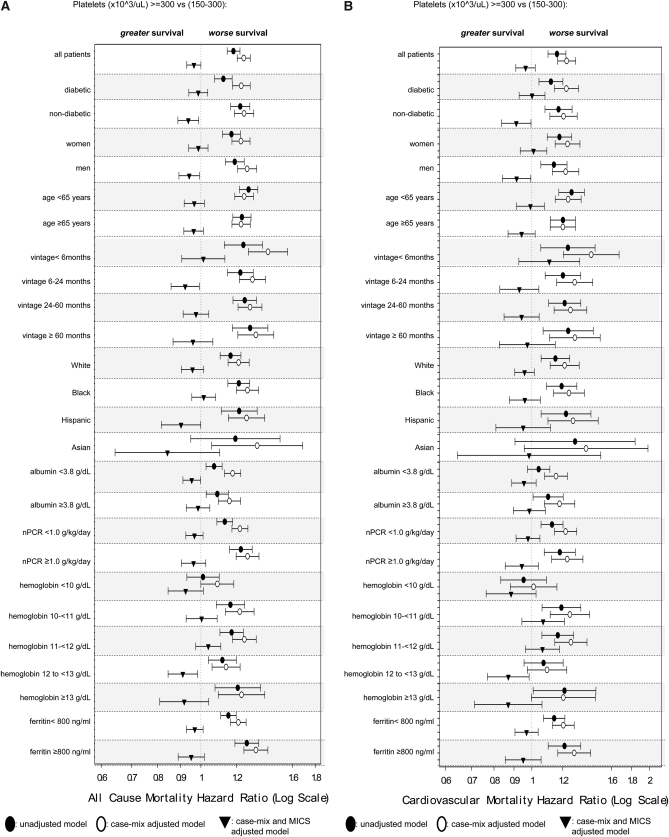
Objectives: We hypothesized that ESRD patients with relative thrombocytosis (platelet count >300 × 10(3)/μL) have a higher mortality rate and that this association may be related to malnutrition-inflammation cachexia syndrome (MICS).
Design: We examined the associations of 3-mo-averaged platelet counts with markers of MICS and 6-y all-cause and cardiovascular mortality (2001-2007) in a cohort of 40,797 patients who were receiving maintenance hemodialysis.
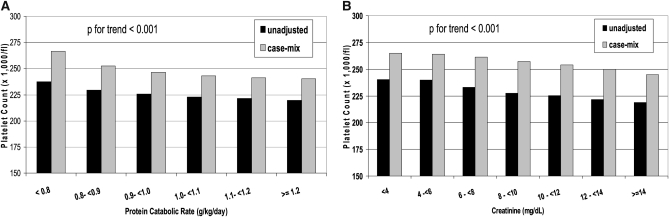
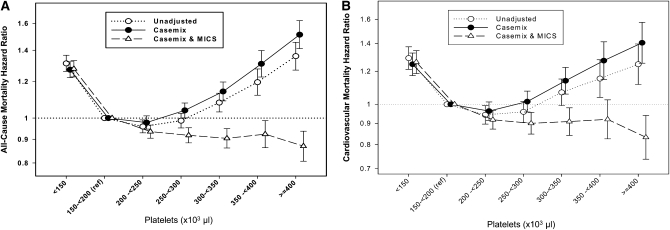
Results: The patients comprised 46% women and 34% African Americans, and 46% of the patients had diabetes. The 3-mo-averaged platelet count was 229 ± 78 × 10(3)/μL. In unadjusted and case-mix adjusted models, lower values of albumin, creatinine, protein intake, hemoglobin, and dialysis dose and a higher erythropoietin dose were associated with a higher platelet count. Compared with patients with a platelet count of between 150 and 200 × 10(3)/μL (reference), the all-cause (and cardiovascular) mortality rate with platelet counts between 300 and <350, between 350 and <400, and ≥400 ×10(3)/μL were 6% (and 7%), 17% (and 15%), and 24% (and 25%) higher (P < 0.05), respectively. The associations persisted after control for case-mix adjustment, but adjustment for MICS abolished them.
Conclusions: Relative thrombocytosis is associated with a worse MICS profile, a lower dialysis dose, and higher all-cause and cardiovascular disease death risk in hemodialysis patients; and its all-cause and cardiovascular mortality predictability is accounted for by MICS. The role of platelet activation in cachexia-associated mortality warrants additional studies.
Figures
References
-
- Coresh J, Astor BC, Greene T, Eknoyan G, Levey AS. Prevalence of chronic kidney disease and decreased kidney function in the adult US population: third National Health and Nutrition Examination Survey. Am J Kidney Dis 2003;41:1–12 - PubMed
-
- Anker SD, Negassa A, Coats AJ, Afzal R, Poole-Wilson PA, Cohn JN, Yusuf S. Prognostic importance of weight loss in chronic heart failure and the effect of treatment with angiotensin-converting-enzyme inhibitors: an observational study. Lancet 2003;361:1077–83 - PubMed
-
- Zile MR, Gaasch WH, Anand IS, Haass M, Little WC, Miller AB, Lopez-Sendon J, Teerlink JR, White M, McMurray JJ, et al. Mode of death in patients with heart failure and a preserved ejection fraction: results from the Irbesartan in Heart Failure With Preserved Ejection Fraction Study (I-Preserve) trial. Circulation 2010;121:1393–405 - PubMed
-
- Aljaroudi WA, Halabi AR, Harrington RA. Platelet inhibitor therapy for patients with cardiovascular disease: looking toward the future. Curr Hematol Rep 2005;4:397–404 - PubMed
