

Exertional dyspnea in mitochondrial myopathy: clinical features and physiological mechanisms
- PMID: 21813873
- PMCID: PMC3197343
- DOI: 10.1152/ajpregu.00001.2011
Exertional dyspnea in mitochondrial myopathy: clinical features and physiological mechanisms
Abstract
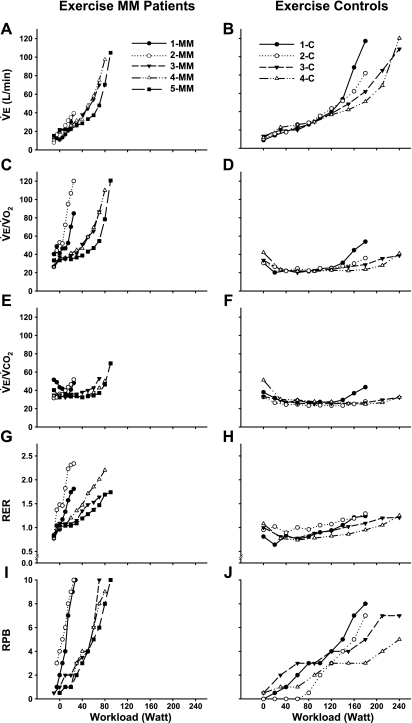
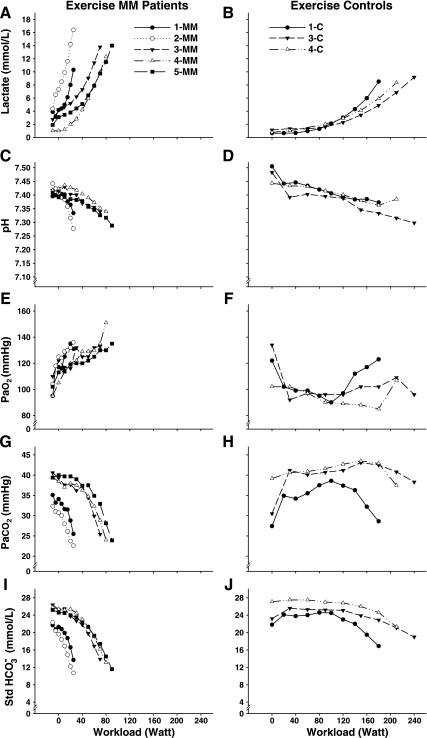
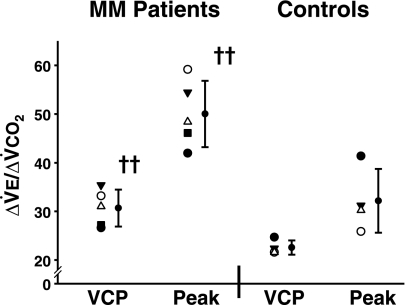
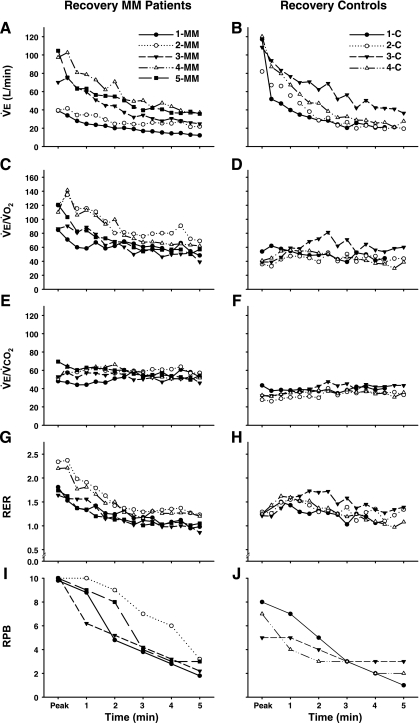
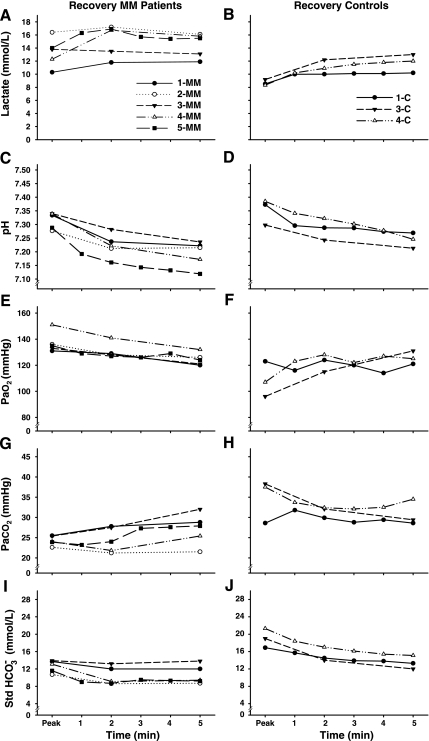
Exertional dyspnea limits exercise in some mitochondrial myopathy (MM) patients, but the clinical features of this syndrome are poorly defined, and its underlying mechanism is unknown. We evaluated ventilation and arterial blood gases during cycle exercise and recovery in five MM patients with exertional dyspnea and genetically defined mitochondrial defects, and in four control subjects (C). Patient ventilation was normal at rest. During exercise, MM patients had low Vo(2peak) (28 ± 9% of predicted) and exaggerated systemic O(2) delivery relative to O(2) utilization (i.e., a hyperkinetic circulation). High perceived breathing effort in patients was associated with exaggerated ventilation relative to metabolic rate with high VE/VO(2peak), (MM = 104 ± 18; C = 42 ± 8, P ≤ 0.001), and Ve/VCO(2peak)(,) (MM = 54 ± 9; C = 34 ± 7, P ≤ 0.01); a steeper slope of increase in ΔVE/ΔVCO(2) (MM = 50.0 ± 6.9; C = 32.2 ± 6.6, P ≤ 0.01); and elevated peak respiratory exchange ratio (RER), (MM = 1.95 ± 0.31, C = 1.25 ± 0.03, P ≤ 0.01). Arterial lactate was higher in MM patients, and evidence for ventilatory compensation to metabolic acidosis included lower Pa(CO(2)) and standard bicarbonate. However, during 5 min of recovery, despite a further fall in arterial pH and lactate elevation, ventilation in MM rapidly normalized. These data indicate that exertional dyspnea in MM is attributable to mitochondrial defects that severely impair muscle oxidative phosphorylation and result in a hyperkinetic circulation in exercise. Exaggerated exercise ventilation is indicated by markedly elevated VE/VO(2), VE/VCO(2), and RER. While lactic acidosis likely contributes to exercise hyperventilation, the fact that ventilation normalizes during recovery from exercise despite increasing metabolic acidosis strongly indicates that additional, exercise-specific mechanisms are responsible for this distinctive pattern of exercise ventilation.
Figures
References
-
- American Thoracic Society Standardization of Spirometry, 1994 Update. American Thoracic Society. Am J Respir Crit Care Med 152: 1107–1136, 1995 - PubMed
-
- Andreu AL, Hanna MG, Reichmann H, Bruno C, Penn AS, Tanji K, Pallotti F, Iwata S, Bonilla E, Lach B, Morgan-Hughes J, DiMauro S. Exercise intolerance due to mutations in the cytochrome b gene of mitochondrial DNA. N Engl J Med 341: 1037–1044, 1999 - PubMed
-
- Anitori R, Manning K, Quan F, Weleber RG, Buist NR, Shoubridge EA, Kennaway NG. Contrasting phenotypes in three patients with novel mutations in mitochondrial tRNA genes. Mol Genet Metab 84: 176–188, 2005 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical