

Comparison of Xpert MTB/RIF with other nucleic acid technologies for diagnosing pulmonary tuberculosis in a high HIV prevalence setting: a prospective study
- PMID: 21814495
- PMCID: PMC3144192
- DOI: 10.1371/journal.pmed.1001061
Comparison of Xpert MTB/RIF with other nucleic acid technologies for diagnosing pulmonary tuberculosis in a high HIV prevalence setting: a prospective study
Abstract
Background: The Xpert MTB/RIF (Cepheid) non-laboratory-based molecular assay has potential to improve the diagnosis of tuberculosis (TB), especially in HIV-infected populations, through increased sensitivity, reduced turnaround time (2 h), and immediate identification of rifampicin (RIF) resistance. In a prospective clinical validation study we compared the performance of Xpert MTB/RIF, MTBDRplus (Hain Lifescience), LightCycler Mycobacterium Detection (LCTB) (Roche), with acid fast bacilli (AFB) smear microscopy and liquid culture on a single sputum specimen.
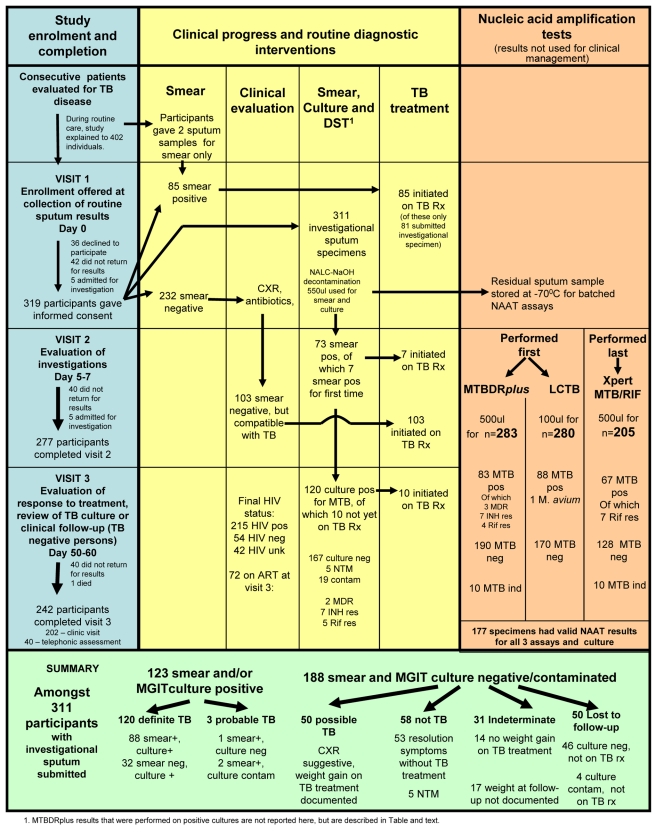
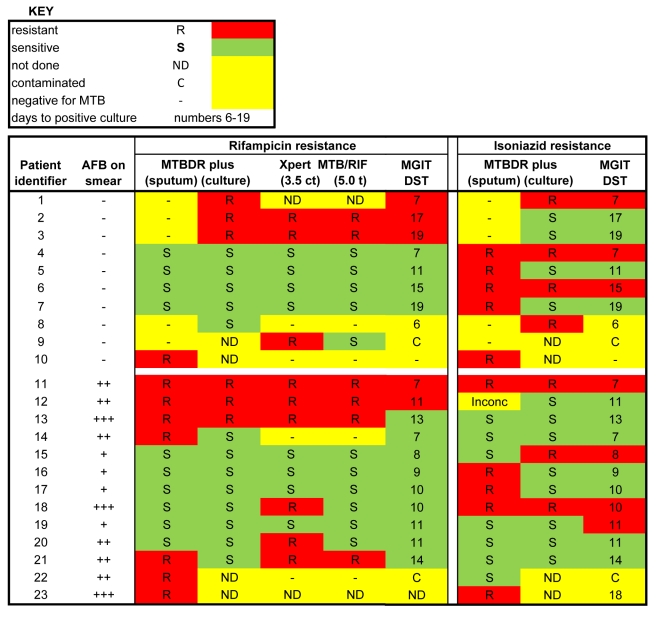
Methods and findings: Consecutive adults with suspected TB attending a primary health care clinic in Johannesburg, South Africa, were prospectively enrolled and evaluated for TB according to the guidelines of the National TB Control Programme, including assessment for smear-negative TB by chest X-ray, clinical evaluation, and HIV testing. A single sputum sample underwent routine decontamination, AFB smear microscopy, liquid culture, and phenotypic drug susceptibility testing. Residual sample was batched for molecular testing. For the 311 participants, the HIV prevalence was 70% (n = 215), with 120 (38.5%) culture-positive TB cases. Compared to liquid culture, the sensitivities of all the test methodologies, determined with a limited and potentially underpowered sample size (n = 177), were 59% (47%-71%) for smear microscopy, 76% (64%-85%) for MTBDRplus, 76% (64%-85%) for LCTB, and 86% (76%-93%) for Xpert MTB/RIF, with specificities all >97%. Among HIV+ individuals, the sensitivity of the Xpert MTB/RIF test was 84% (69%-93%), while the other molecular tests had sensitivities reduced by 6%. TB detection among smear-negative, culture-positive samples was 28% (5/18) for MTBDRplus, 22% (4/18) for LCTB, and 61% (11/18) for Xpert MTB/RIF. A few (n = 5) RIF-resistant cases were detected using the phenotypic drug susceptibility testing methodology. Xpert MTB/RIF detected four of these five cases (fifth case not tested) and two additional phenotypically sensitive cases.
Conclusions: The Xpert MTB/RIF test has superior performance for rapid diagnosis of Mycobacterium tuberculosis over existing AFB smear microscopy and other molecular methodologies in an HIV- and TB-endemic region. Its place in the clinical diagnostic algorithm in national health programs needs exploration. Please see later in the article for the Editors' Summary.
Conflict of interest statement
The Academic Editor, Madhukar Pai, declares that he consults for the Bill & Melinda Gates Foundation (BMGF). The BMGF supported the Foundation for Innovative New Diagnostics (FIND), which was involved in the development of the Xpert MTB/RIF assay. He also co-chairs the Stop TB Partnership's New Diagnostics Working Group that was involved in the WHO endorsement of the Xpert assay. The authors have declared that no competing interests exist.
Figures
References
-
- Averting HIV AIDS. HIV and AIDS in South Africa. West Sussex (United Kingdom): Averting HIV and AIDS; 2010. Available: http://www.avert.org/aidssouthafrica.htm. Accessed 15 June 2011.
-
- United States Agency for International Development. South Africa: HIV/AIDS health profile. Pretoria: USAID/South Africa; 2011. Available: http://www.usaid.gov/our_work/global_health/aids/Countries/africa/southa.... Accessed 27 June 2011.
-
- World Health Organization. Global tuberculosis control: epidemiology, strategy, financing. Geneva: World Health Organization; 2009.
-
- Ndjeka N. Policy framework for decentralization of MDR-TB services [presentation]. 2011. Aurum Institute Tembisa TB Symposium.
-
- Cohen T, Murray M, Wallengren K, Alvarez GG, Samuel EY, et al. The prevalence and drug sensitivity of tuberculosis among patients dying in hospital in KwaZulu-Natal, South Africa: a postmortem study. PLoS Med. 2010;7:e1000296. doi: 10.1371/journal.pmed.1000296. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
