

Referral patterns and outcomes in noncritically ill patients with hospital-acquired acute kidney injury
- PMID: 21817132
- PMCID: PMC3359001
- DOI: 10.2215/CJN.01880211
Referral patterns and outcomes in noncritically ill patients with hospital-acquired acute kidney injury
Abstract
Background and objectives: Despite modern treatment, the case fatality rate of hospital-acquired acute kidney injury (HA-AKI) is still high. We retrospectively described the prevalence and the outcome of HA-AKI without nephrology referral (nrHA-AKI) and late referred HA-AKI patients to nephrologists (lrHA-AKI) compared with early referral patients (erHA-AKI) with respect to renal function recovery, renal replacement therapy (RRT) requirement, and in-hospital mortality of HA-AKI.
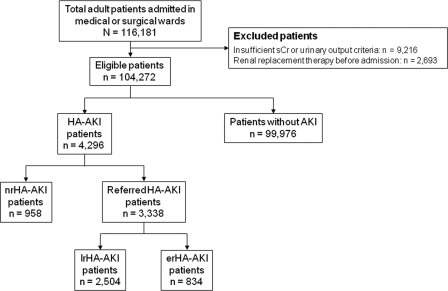
Design, setting, participants, & measurements: Noncritically ill patients admitted to the tertiary care academic center of Lausanne, Switzerland, between 2004 and 2008 in the medical and surgical services were included. Acute kidney injury was defined using the Acute Kidney Injury Network (AKIN) classification.
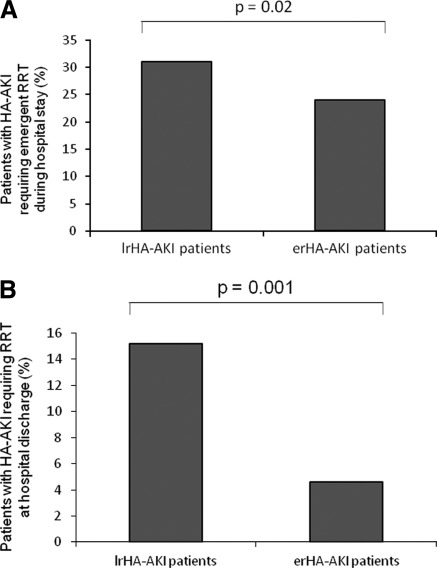
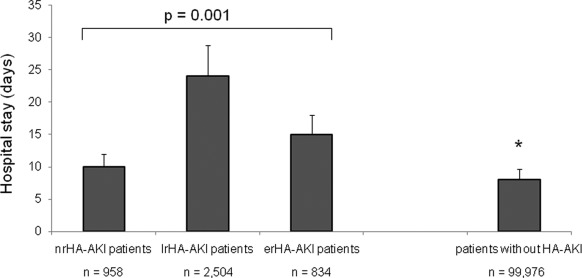
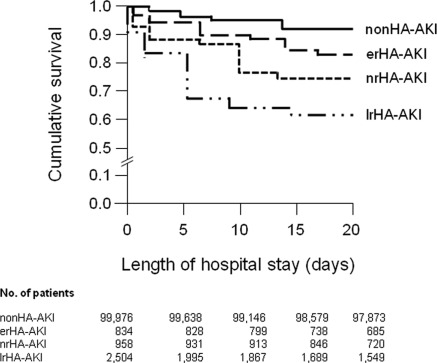
Results: During 5 years, 4296 patients (4.12% of admissions) experienced 4727 episodes of HA-AKI during their hospital stay. The mean ± SD age of the patients was 61 ± 15 years with a 55% male predominance. There were 958 patients with nrHA-AKI (22.3%) and 2504 patients with lrHA-AKI (58.3%). RRT was required in 31% of the patients with lrHA-AKI compared with 24% of the patients with erHA-AKI. In the multiple risk factor analysis, compared with erHA-AKI, nrHA-AKI and lrHA-AKI were significantly associated with worse renal outcome and higher in-hospital mortality.
Conclusions: These data suggest that HA-AKI is frequent and the patients with nrHA-AKI or lrHA-AKI are at increased risk for in-hospital morbidity and mortality.
Figures
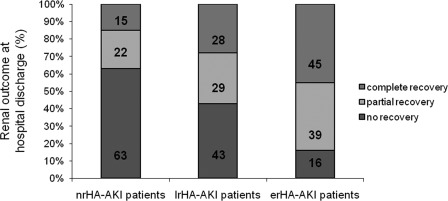
 , percentage of patients with complete recovery (>75% ΔSCr);
, percentage of patients with complete recovery (>75% ΔSCr);  , percentage of patients with partial recovery (25% to 75% ΔSCr); ■, percentage of patients with no recovery (<25% ΔSCr). P = 0.001. nrHA-AKI, hospital-acquired acute kidney injury; without nephrology referral; lrHA-AKI, late-referred HA-AKI; erHA-AKI, early-referred HA-AKI.
, percentage of patients with partial recovery (25% to 75% ΔSCr); ■, percentage of patients with no recovery (<25% ΔSCr). P = 0.001. nrHA-AKI, hospital-acquired acute kidney injury; without nephrology referral; lrHA-AKI, late-referred HA-AKI; erHA-AKI, early-referred HA-AKI.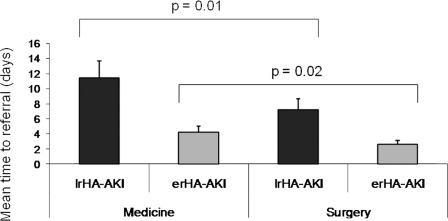
Comment in
-
Management of acute kidney injury: it's the squeaky wheel that gets the oil!Clin J Am Soc Nephrol. 2011 Sep;6(9):2102-4. doi: 10.2215/CJN.07720811. Epub 2011 Aug 18. Clin J Am Soc Nephrol. 2011. PMID: 21852670 No abstract available.
References
-
- Ricci Z, Cruz D, Ronco C: The RIFLE criteria and mortality in acute kidney injury: A systematic review. Kidney Int 73: 538–546, 2008 - PubMed
-
- Kwon SH, Noh H, Jeon JS, Kim Y, Han DC: An assessment of AKIN criteria for hospital-acquired acute kidney injury: A prospective observational cohort study. Nephron Clin Pract 116: 217–223, 2010 - PubMed
-
- Hou SH, Bushinsky DA, Wish JB, Cohen JJ, Harrington JT: Hospital-acquired renal insufficiency: A prospective study. Am J Med 74: 243–248, 1983 - PubMed
-
- Shusterman N, Strom BL, Murray TG, Morrison G, West SL, Maislin G: Risk factors and outcome of hospital-acquired acute renal failure. Am J Med 83: 65–71, 1987 - PubMed
-
- Nash K, Hafeez A, Hou S: Hospital-acquired renal insufficiency. Am J Kidney Dis 39: 930–936, 2002 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
