

Thoracolumbar imbalance analysis for osteotomy planification using a new method: FBI technique
- PMID: 21818597
- PMCID: PMC3175920
- DOI: 10.1007/s00586-011-1935-y
Thoracolumbar imbalance analysis for osteotomy planification using a new method: FBI technique
Abstract
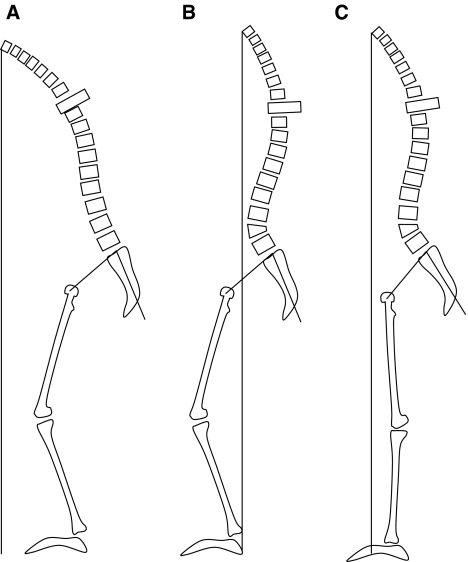
Introduction: Treatment of spine imbalance by posterior osteotomy is a valuable technique. Several surgical techniques have been developed and proposed to redress the vertebral column in harmonious kyphosis in order to recreate correct sagittal alignment. Although surgical techniques proved to be adequate, preoperative planning still is mediocre. Multiple suggestions have been proposed, from cutting tracing paper to ingenious mathematical formulas and computerised models. The analysis of the pelvic parameters to try to recover the initial shape of the spine before the spine imbalance occurred is very important to avoid mistakes during the osteotomy planification.
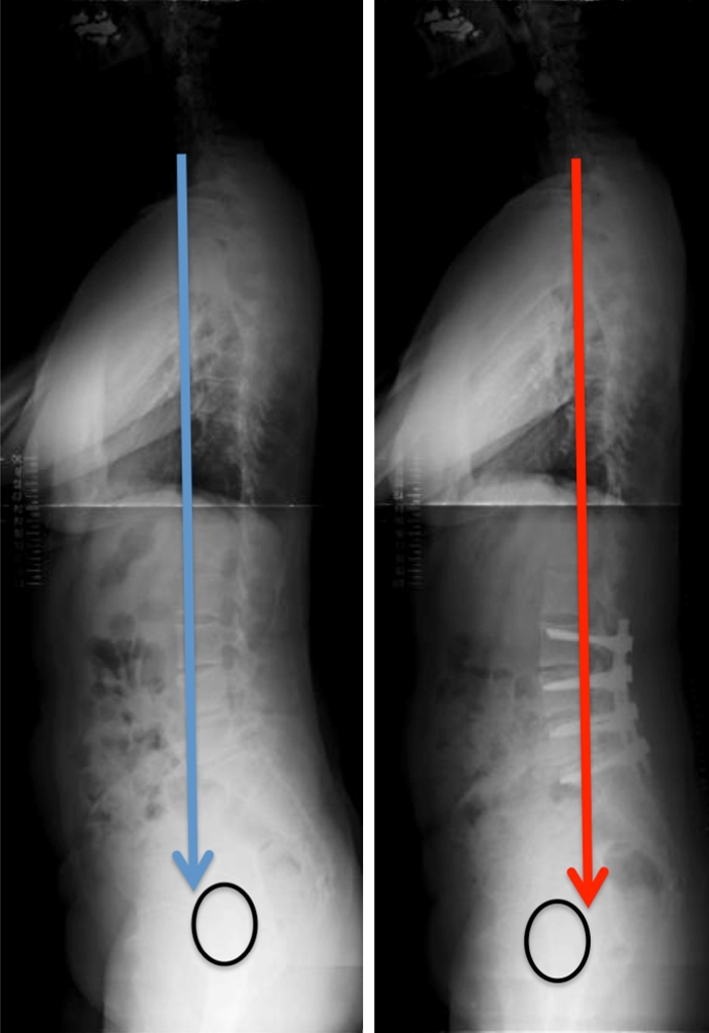
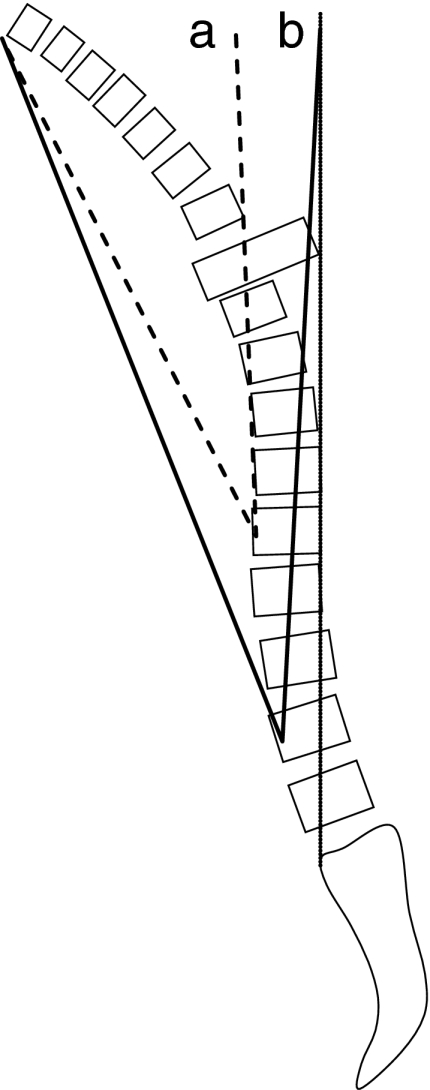
Material and method: The authors proposed their method for the osteotomy planning paying attention to the pelvic, and spine parameters and in accordance with Roussouly's classification. The pre operative planning is based on a full-body X-ray including the spine from C1 to the femoral head and the first 10 cm of the femur shaft. Using all the balance parameters provided, a formula name FBI is proposed. Calculation of the osteotomy is basic goniometry, the midpoint of the C7 inferior plateau (point a) is transposed horizontally on the projected future C7 plumb line (point b) crossing posterior S1 plateau on a sagittal X-ray. These are the first two reference points. A third reference point is made on the anterior wall of the selected vertebra for osteotomy at mid height of the pedicle (point c) mainly L4 vertebra. These three points form a triangle with the tip being the third reference point. The angle represented by this triangle is the theoretical angle of the osteotomy. Two more angles should be measured and eventually added. The femur angulation measured as the inclination of the femoral axis to the vertical. And a third angle named the compensatory pelvic tilt to integrate the type of pelvis. If the pelvic tilt is between 15 and 25° or is higher than 25° you must add 5 or 10°, respectively. This compensatory tilt is based on a clinical analysis of operated patients.
Results: This planification was applied in a retrospective study of 18 patients and showed why in some cases improper correction was performed and prospectively in 8 cases with good clinical outcomes and correct spinal alignment. Sometimes it is necessary to find an acceptable compromise when rebalancing the spine paying attention to the general parameters of the patients like: age, osteoporosis, systemic disease etc.
Conclusion: This FBI technique can be used even for small lordosis restoration: it gave a good evaluation of the amount of correction needed and then the surgeon had the choice to use the appropriate technique to obtain a good balance.
Figures






References
-
- Aurouer N, Obeid I, Gille O, Pointillart V, Vital JM (2009) Computerized preoperative planning for correction of sagittal deformity of the spine. Surg Radiol Anat, Jul 14. [Epub ahead of print] - PubMed
-
- Bridwell KH, Lewis SJ, Lenke LG, Baldus C, Blanke K. Pedicle subtraction osteotomy for the treatment of fixed sagittal imbalance. J Bone Joint Surg Am. 2003;85-A(3):454–463. - PubMed
-
- Bridwell KH, Lewis SJ, Rinella A, Lenke LG, Baldus C, Blanke K. Pedicle subtraction osteotomy for the treatment of fixed sagittal imbalance. Surgical technique. J Bone Joint Surg Am. 2004;86-A(Suppl 1):44–50. - PubMed
-
- Burton DC. Smith-Petersen osteotomy of the spine. Instr Course Lect. 2006;55:577–582. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
