

Using verbal autopsy to track epidemic dynamics: the case of HIV-related mortality in South Africa
- PMID: 21819601
- PMCID: PMC3160939
- DOI: 10.1186/1478-7954-9-46
Using verbal autopsy to track epidemic dynamics: the case of HIV-related mortality in South Africa
Abstract
Background: Verbal autopsy (VA) has often been used for point estimates of cause-specific mortality, but seldom to characterize long-term changes in epidemic patterns. Monitoring emerging causes of death involves practitioners' developing perceptions of diseases and demands consistent methods and practices. Here we retrospectively analyze HIV-related mortality in South Africa, using physician and modeled interpretation.
Methods: Between 1992 and 2005, 94% of 6,153 deaths which occurred in the Agincourt subdistrict had VAs completed, and coded by two physicians and the InterVA model. The physician causes of death were consolidated into a single consensus underlying cause per case, with an additional physician arbitrating where different diagnoses persisted. HIV-related mortality rates and proportions of deaths coded as HIV-related by individual physicians, physician consensus, and the InterVA model were compared over time.
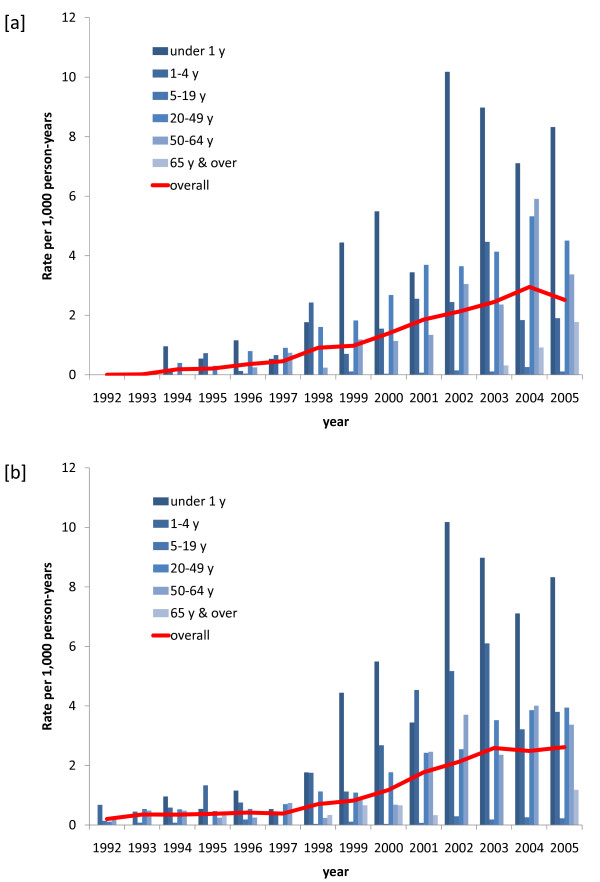
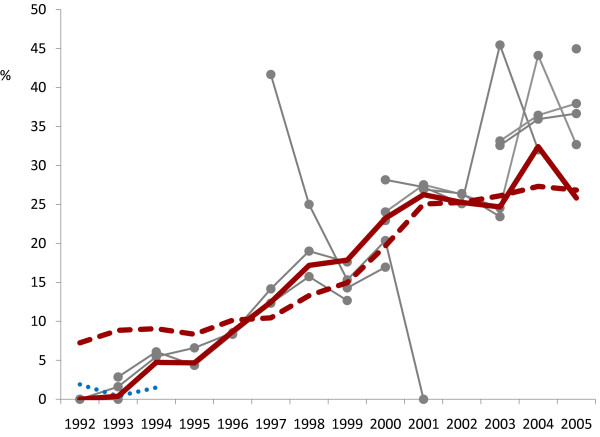
Results: Approximately 20% of deaths were HIV-related, ranging from early low levels to tenfold-higher later population rates (2.5 per 1,000 person-years). Rates were higher among children under 5 years and adults 20 to 64 years. Adult mortality shifted to older ages as the epidemic progressed, with a noticeable number of HIV-related deaths in the over-65 year age group latterly. Early InterVA results suggested slightly higher initial HIV-related mortality than physician consensus found. Overall, physician consensus and InterVA results characterized the epidemic very similarly. Individual physicians showed marked interobserver variation, with consensus findings generally reflecting slightly lower proportions of HIV-related deaths. Aggregated findings for first versus second physician did not differ appreciably.
Conclusions: VA effectively detected a very significant epidemic of HIV-related mortality. Using either physicians or InterVA gave closely comparable findings regarding the epidemic. The consistency between two physician coders per case (from a pool of 14) suggests that double coding may be unnecessary, although the consensus rate of HIV-related mortality was approximately 8% lower than by individual physicians. Consistency within and between individual physicians, individual perceptions of epidemic dynamics, and the inherent consistency of models are important considerations here. The ability of the InterVA model to track a more than tenfold increase in HIV-related mortality over time suggests that finely tuned "local" versions of models for VA interpretation are not necessary.
Figures
Similar articles
-
Causes and circumstances of maternal death: a secondary analysis of the Community-Level Interventions for Pre-eclampsia (CLIP) trials cohort.Lancet Glob Health. 2021 Sep;9(9):e1242-e1251. doi: 10.1016/S2214-109X(21)00263-1. Epub 2021 Jul 29. Lancet Glob Health. 2021. PMID: 34332699 Free PMC article. Clinical Trial.
-
Validity of InterVA model versus physician review of verbal autopsy for tracking tuberculosis-related mortality in Ethiopia.BMC Infect Dis. 2022 Mar 1;22(1):200. doi: 10.1186/s12879-022-07193-w. BMC Infect Dis. 2022. PMID: 35232392 Free PMC article.
-
Moving from data on deaths to public health policy in Agincourt, South Africa: approaches to analysing and understanding verbal autopsy findings.PLoS Med. 2010 Aug 17;7(8):e1000325. doi: 10.1371/journal.pmed.1000325. PLoS Med. 2010. PMID: 20808956 Free PMC article.
-
Validation of verbal autopsy methods for assessment of child mortality in sub-Saharan Africa and the policy implication: a rapid review.Pan Afr Med J. 2019 Aug 22;33:318. doi: 10.11604/pamj.2019.33.318.16405. eCollection 2019. Pan Afr Med J. 2019. PMID: 31692720 Free PMC article. Review.
-
Verbal autopsy models in determining causes of death.Trop Med Int Health. 2021 Dec;26(12):1560-1567. doi: 10.1111/tmi.13678. Epub 2021 Sep 30. Trop Med Int Health. 2021. PMID: 34498340
Cited by
-
Strengthening standardised interpretation of verbal autopsy data: the new InterVA-4 tool.Glob Health Action. 2012 Sep 3;5:1-8. doi: 10.3402/gha.v5i0.19281. Glob Health Action. 2012. PMID: 22944365 Free PMC article.
-
Validating the InterVA model to estimate the burden of mortality from verbal autopsy data: a population-based cross-sectional study.PLoS One. 2013 Sep 13;8(9):e73463. doi: 10.1371/journal.pone.0073463. eCollection 2013. PLoS One. 2013. PMID: 24058474 Free PMC article.
-
The development of a localised HIV epidemic and the associated excess mortality burden in a rural area of South Africa.Glob Health Epidemiol Genom. 2016 Mar 23;1:e7. doi: 10.1017/gheg.2016.3. eCollection 2016. Glob Health Epidemiol Genom. 2016. PMID: 29302331 Free PMC article.
-
Disease-specific mortality burdens in a rural Gambian population using verbal autopsy, 1998-2007.Glob Health Action. 2014 Oct 29;7:25598. doi: 10.3402/gha.v7.25598. eCollection 2014. Glob Health Action. 2014. PMID: 25377344 Free PMC article.
-
Essential evidence for guiding health system priorities and policies: anticipating epidemiological transition in Africa.Glob Health Action. 2014 May 15;7:23359. doi: 10.3402/gha.v7.23359. eCollection 2014. Glob Health Action. 2014. PMID: 24848653 Free PMC article.
References
-
- Joint United Nations Program on HIV/AIDS. Global report: UNAIDS report on the global AIDS epidemic 2010. Geneva: UNAIDS; 2010. http://www.unaids.org/en/media/unaids/contentassets/documents/unaidspubl... ISBN 978-92-9173-871-7.
-
- Dorrington RE, Johnson LF, Bradshaw D, Daniel T. The Demographic Impact of HIV/AIDS in South Africa. National and Provincial Indicators for 2006. Cape Town: Centre for Actuarial Research, South African Medical Research Council and Actuarial Society of South Africa; 2006. http://www.mrc.ac.za/bod/DemographicImpactHIVIndicators.pdf
LinkOut - more resources
Full Text Sources
