

Growth of preschool children at high risk for asthma 2 years after discontinuation of fluticasone
- PMID: 21820163
- PMCID: PMC3224818
- DOI: 10.1016/j.jaci.2011.06.027
Growth of preschool children at high risk for asthma 2 years after discontinuation of fluticasone
Abstract
Background: The effect on linear growth of daily long-term inhaled corticosteroid therapy in preschool-aged children with recurrent wheezing is controversial.
Objective: We sought to determine the effect of daily inhaled corticosteroid given for 2 years on linear growth in preschool children with recurrent wheezing.
Methods: Children aged 2 and 3 years with recurrent wheezing and positive modified Asthma Predictive Index scores were randomized to a 2-year treatment period of chlorofluorocarbon-delivered fluticasone propionate (176 μg/d) or masked placebo delivered through a valved chamber with a mask and then followed for 2 years off study medication. Height growth determined by means of stadiometry was compared between treatment groups.
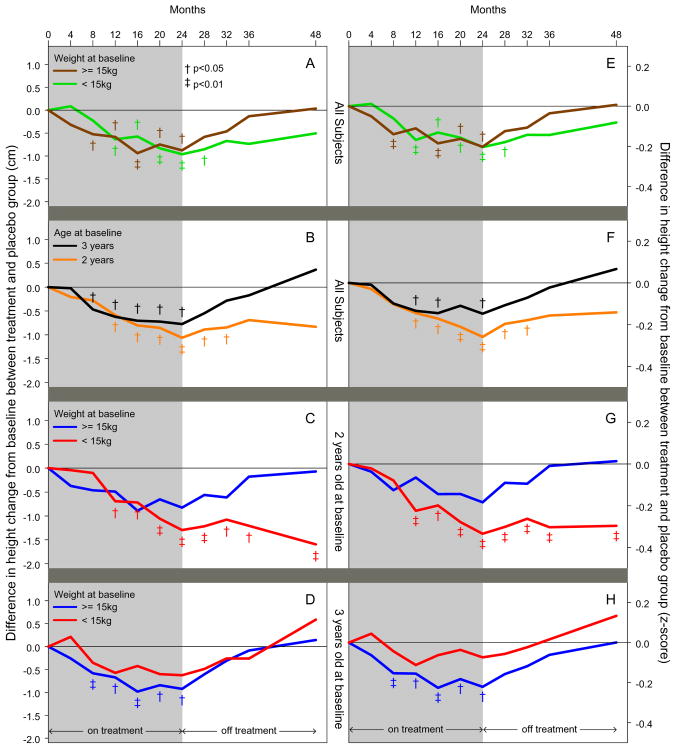
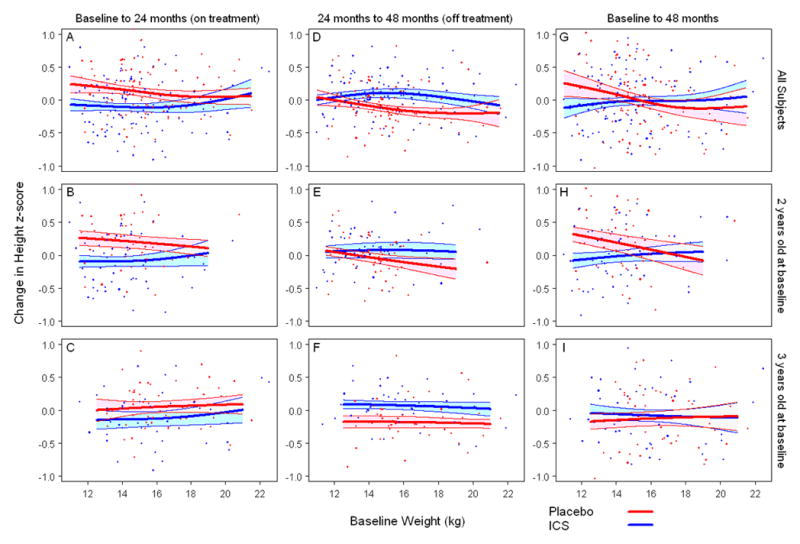
Results: In the study cohort as a whole, the fluticasone group did not have significantly less linear growth than the placebo group (change in height from baseline difference, -0.2 cm; 95% CI, -1.1 to 0.6) 2 years after discontinuation of study treatment. In post hoc analyses children 2 years old who weighed less than 15 kg at enrollment and were treated with fluticasone had less linear growth compared with those treated with placebo (change in height from baseline difference, -1.6 cm; 95% CI, -2.8 to -0.4; P = .009).
Conclusion: Linear growth was not significantly different in high-risk preschool-aged children with recurrent wheezing treated with 176 μg/d chlorofluorocarbon-delivered fluticasone compared with placebo 2 years after fluticasone is discontinued. However, post hoc subgroup analyses revealed that children who are younger in age and of lesser weight relative to the entire study cohort had significantly less linear growth, possibly because of a higher relative fluticasone exposure.
Copyright © 2011 American Academy of Allergy, Asthma & Immunology. Published by Mosby, Inc. All rights reserved.
Figures
References
-
- Agertoft L, Pedersen S. Effect of long-term treatment with inhaled budesonide on adult height in children with asthma. N Engl J Med. 2000 Oct 12;343(15):1064–9. - PubMed
-
- The Childhood Asthma Management Program Research Group. Long-term effects of budesonide or nedocromil in children with asthma. N Engl J Med. 2000 Oct 12;343(15):1054–63. - PubMed
-
- Guilbert TW, Morgan WJ, Zeiger RS, Mauger DT, Boehmer SJ, Szefler SJ, et al. Long-term inhaled corticosteroids in preschool children at high risk for asthma. N Engl J Med. 2006 May 11;354(19):1985–97. - PubMed
-
- Guilbert TW, Morgan WJ, Krawiec M, Lemanske RF, Jr, Sorkness C, Szefler SJ, et al. The Prevention of Early Asthma in Kids study: design, rationale and methods for the Childhood Asthma Research and Education network. Control Clin Trials. 2004 Jun;25(3):286–310. - PubMed
-
- Castro-Rodriguez JA, Holberg CJ, Wright AL, Martinez FD. A clinical index to define risk of asthma in young children with recurrent wheezing. Am J Respir Crit Care Med. 2000 Oct;162(4 Pt 1):1403–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- HL004519-04/HL/NHLBI NIH HHS/United States
- 5U10HL064305/HL/NHLBI NIH HHS/United States
- UL1 RR025780/RR/NCRR NIH HHS/United States
- K08 HL071742/HL/NHLBI NIH HHS/United States
- U10 HL064295/HL/NHLBI NIH HHS/United States
- 5U10HL064313/HL/NHLBI NIH HHS/United States
- U10 HL064305/HL/NHLBI NIH HHS/United States
- 5U10HL064295/HL/NHLBI NIH HHS/United States
- 1 UL1 RR025780/RR/NCRR NIH HHS/United States
- U10 HL064313/HL/NHLBI NIH HHS/United States
- U10 HL064307/HL/NHLBI NIH HHS/United States
- M01 RR000036/RR/NCRR NIH HHS/United States
- U10 HL064288/HL/NHLBI NIH HHS/United States
- K30 HL004519/HL/NHLBI NIH HHS/United States
- U10 HL064287/HL/NHLBI NIH HHS/United States
- 5U10HL064307/HL/NHLBI NIH HHS/United States
- 5U10HL064288/HL/NHLBI NIH HHS/United States
- HL071742/HL/NHLBI NIH HHS/United States
- M01 RR00036/RR/NCRR NIH HHS/United States
- 5U10HL064287/HL/NHLBI NIH HHS/United States
