

Post-operative atrial fibrillation: a maze of mechanisms
- PMID: 21821851
- PMCID: PMC3262403
- DOI: 10.1093/europace/eur208
Post-operative atrial fibrillation: a maze of mechanisms
Abstract
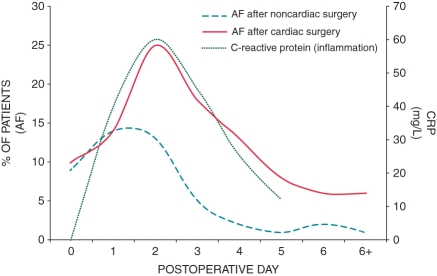
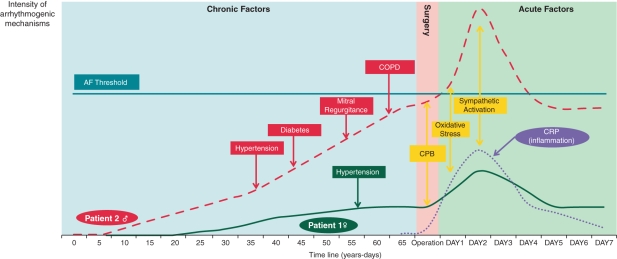
Post-operative atrial fibrillation (POAF) is one of the most frequent complications of cardiac surgery and an important predictor of patient morbidity as well as of prolonged hospitalization. It significantly increases costs for hospitalization. Insights into the pathophysiological factors causing POAF have been provided by both experimental and clinical investigations and show that POAF is 'multi-factorial'. Facilitating factors in the mechanism of the arrhythmia can be classified as acute factors caused by the surgical intervention and chronic factors related to structural heart disease and ageing of the heart. Furthermore, some proarrhythmic mechanisms specifically occur in the setting of POAF. For example, inflammation and beta-adrenergic activation have been shown to play a prominent role in POAF, while these mechanisms are less important in non-surgical AF. More recently, it has been shown that atrial fibrosis and the presence of an electrophysiological substrate capable of maintaining AF also promote the arrhythmia, indicating that POAF has some proarrhythmic mechanisms in common with other forms of AF. The clinical setting of POAF offers numerous opportunities to study its mechanisms. During cardiac surgery, biopsies can be taken and detailed electrophysiological measurements can be performed. Furthermore, the specific time course of POAF, with the delayed onset and the transient character of the arrhythmia, also provides important insight into its mechanisms. This review discusses the mechanistic interaction between predisposing factors and the electrophysiological mechanisms resulting in POAF and their therapeutic implications.
Figures
References
-
- Creswell LL, Schuessler RB, Rosenbloom M, Cox JL. Hazards of postoperative atrial arrhythmias. Ann Thorac Surg. 1993;56:539–49. - PubMed
-
- Mathew JP, Fontes ML, Tudor IC, Ramsay J, Duke P, Mazer CD, et al. A multicenter risk index for atrial fibrillation after cardiac surgery. JAMA. 2004;291:1720–9. - PubMed
-
- Aranki SF, Shaw DP, Adams DH, Rizzo RJ, Couper GS, VanderVliet M, et al. Predictors of atrial fibrillation after coronary artery surgery. Current trends and impact on hospital resources. Circulation. 1996;94:390–7. - PubMed
-
- Frost L, Molgaard H, Christiansen EH, Hjortholm K, Paulsen PK, Thomsen PE. Atrial fibrillation and flutter after coronary artery bypass surgery: epidemiology, risk factors and preventive trials. Int J Cardiol. 1992;36:253–61. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
