

Gray zone lymphoma: chromosomal aberrations with immunophenotypic and clinical correlations
- PMID: 21822207
- PMCID: PMC6368823
- DOI: 10.1038/modpathol.2011.116
Gray zone lymphoma: chromosomal aberrations with immunophenotypic and clinical correlations
Abstract
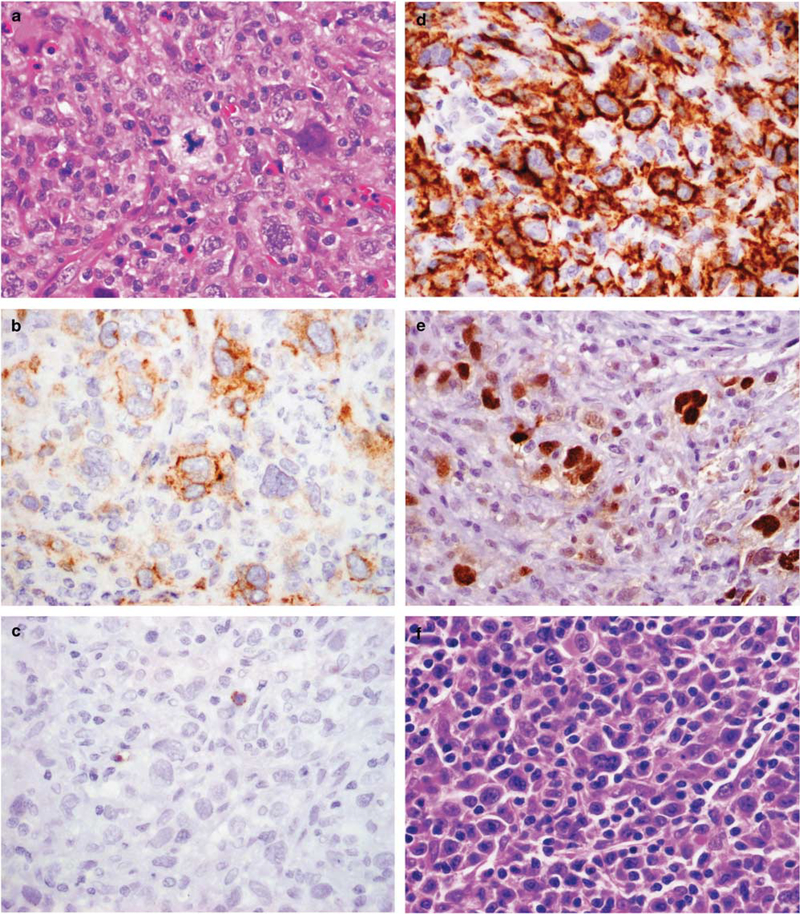
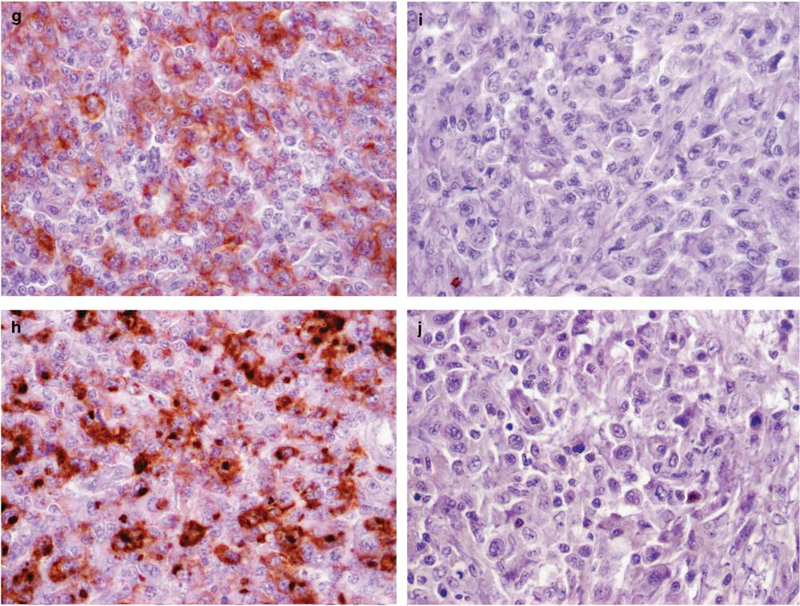
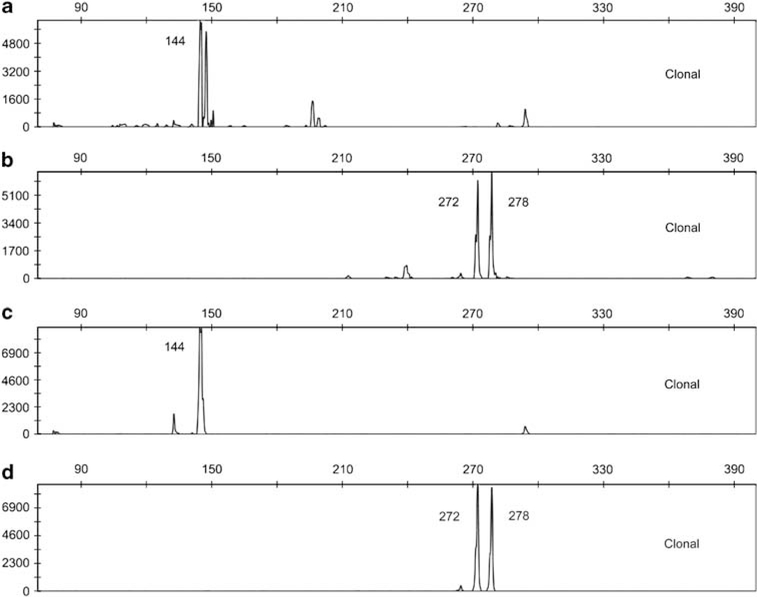
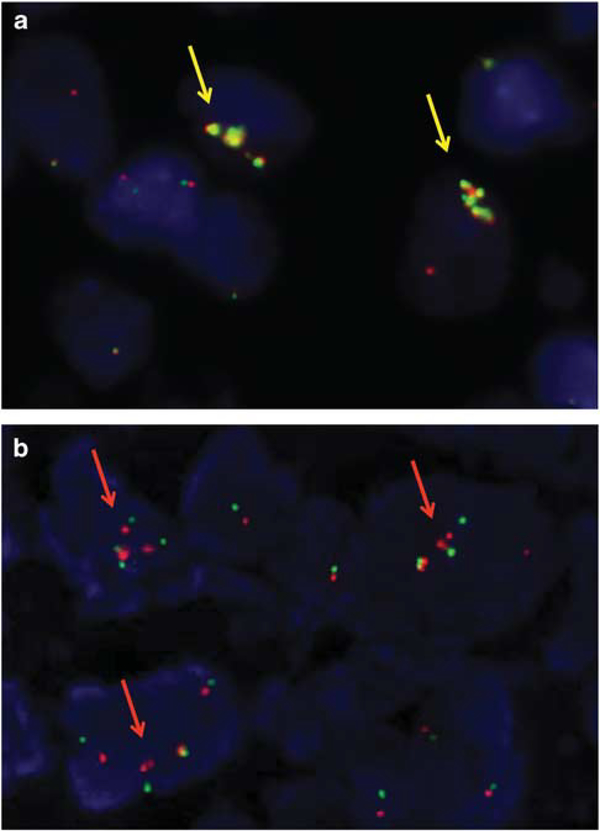
The term gray zone lymphoma has been applied to tumors that demonstrate transitional morphologic and immunophenotypic features between classical Hodgkin's lymphoma and diffuse large B-cell lymphoma, especially primary mediastinal large B-cell lymphoma. Histopathological and genetic data are limited for these unusual cases. We analyzed cases of gray zone lymphoma (n=27), mediastinal composite lymphoma (n=3) and mediastinal synchronous/metachronous lymphoma (n=3) by morphology, immunophenotyping and fluorescence in situ hybridization. Mediastinal involvement was assured in 24/33 patients (73%). The patient cohort showed a male predominance (M:F ratio; 20:13) and a median age of 32 years (range, 16-91 years). Patients with mediastinal disease were significantly younger (median age: 29.5 years) than patients presenting without evident mediastinal disease (median age: 55 years). Gains including amplifications in 2p16.1 (REL/BCL11A locus) were observed in 33% of all patients, whereas alterations affecting the JAK2/PDL2 locus in 9p24.1 were present in 55%. Further studies revealed rearrangement of the CIITA locus at 16p13.13 in 8/30 cases (27%) and 7/26 cases (27%) demonstrated gains of 8q24 (MYC). Genetic aberrations involving 2p16.1, 9p24.1 and 8q24 showed a higher incidence in cases with evident mediastinal involvement. However, this was not statistically significant when compared with cases without known mediastinal involvement. Twelve of the 27 cases of gray zone lymphoma were morphologically more reminiscent of classical Hodgkin's lymphoma, whereas the other gray zone lymphomas presented with morphological features more closely resembling large B-cell lymphoma. Both morphological groups of gray zone lymphoma were similarly positive for Cyclin E (75 and 93%) and p63 (50 and 53%, respectively) expression. These findings further support a close relationship between gray zone lymphoma, classical Hodgkin's lymphoma and primary mediastinal large B-cell lymphoma, and suggest that some cases of gray zone lymphoma without mediastinal disease may share similar genetic alterations.
Conflict of interest statement
Disclosure/conflict of interest
The authors declare no conflict of interest.
Figures
References
-
- Perrone T, Frizzera G, Rosai J. Mediastinal diffuse large-cell lymphoma with sclerosis. A clinicopathologic study of 60 cases. Am J Surg Pathol 1986;10: 176–191. - PubMed
-
- Gonzalez CL, Medeiros LJ, Jaffe ES. Composite lymphoma. A clinicopathologic analysis of nine patients with Hodgkin’s disease and B-cell non-Hodgkin’s lymphoma. Am J Clin Pathol 1991;96:81–89. - PubMed
-
- Zarate-Osorno A, Medeiros LJ, Longo DL, et al. Non-Hodgkin’s lymphomas arising in patients successfully treated for Hodgkin’s disease. A clinical, histologic, and immunophenotypic study of 14 cases. Am J Surg Pathol 1992;16:885–895. - PubMed
-
- Zarate-Osorno A, Medeiros LJ, Kingma DW, et al. Hodgkin’s disease following non-Hodgkin’s lymphoma. A clinicopathologic and immunophenotypic study of nine cases. Am J Surg Pathol 1993;17:123–132. - PubMed
-
- Garcia JF, Mollejo M, Fraga M, et al. Large B-cell lymphoma with Hodgkin’s features. Histopathology 2005;47:101–110. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
