

Stem and osteotomy length are critical for success of the transfemoral approach and cementless stem revision
- PMID: 21822571
- PMCID: PMC3270197
- DOI: 10.1007/s11999-011-1998-4
Stem and osteotomy length are critical for success of the transfemoral approach and cementless stem revision
Abstract
Background: The transfemoral approach is an extensile surgical approach that is performed routinely to facilitate cement and implant removal and improve exposure for revision stem implantation. Previous studies have looked at clinical results of small patient groups. The factors associated with fixation failure of cementless revision stems when using this approach have not been examined.
Questions/purposes: We determined (1) the clinical results and (2) complications of the transfemoral approach and (3) factors associated with fixation failure of revision stems when using the transfemoral approach.
Patients and methods: We retrospectively examined all our patients in whom femoral stem revision was performed through a transfemoral approach between December 1998 and April 2004 and for whom a minimal followup of 2 years was available. One hundred patients were available for this study. The mean (± SD) postoperative followup was 5 years (± 1.64 years).
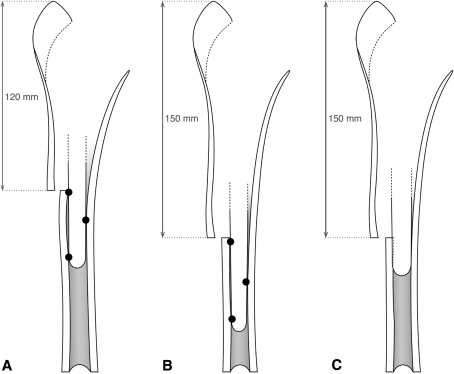
Results: The average Harris hip score improved from 45.2 (± 14.02) preoperatively to 83.4 (± 11.86) at final followup. Complete radiographic bony consolidation of the osteotomy site was observed in 95% of patients. Dislocations occurred in 9% of patients. Four revision stem fixation failures were observed, all occurring in patients with primary three-point fixation. Three-point fixation was associated with short osteotomy flaps and long revision stems.
Conclusions: The transfemoral approach is associated with a high rate of osteotomy flap bony healing and good clinical results. When using the transfemoral approach, a long osteotomy flap should be performed and the shortest possible revision stem should be implanted.
Level of evidence: Level IV, therapeutic study. See Guidelines for Authors for a complete description of levels of evidence.
Figures


References
-
- Amstutz HC, Maki S. Complications of trochanteric osteotomy in total hip replacement. J Bone Joint Surg Am. 1978;60:214–216. - PubMed
-
- Boisgard S, Moreau PE, Tixier H, Levai JP. Bone reconstruction, leg length discrepancy, and dislocation rate in 52 Wagner revision total hip arthroplasties at 44-month follow-up] [in French] Rev Chir Orthop Reparatrice Appar Mot. 2001;87:147–154. - PubMed
-
- Chen WM, McAuley JP, Engh CA, Jr, Hopper RH, Jr, Engh CA. Extended slide trochanteric osteotomy for revision total hip arthroplasty. J Bone Joint Surg Am. 2000;82:1215–1219. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
