

Comparison of the puborectal muscle on MRI in women with POP and levator ani defects with those with normal support and no defect
- PMID: 21822711
- PMCID: PMC3508430
- DOI: 10.1007/s00192-011-1527-8
Comparison of the puborectal muscle on MRI in women with POP and levator ani defects with those with normal support and no defect
Abstract
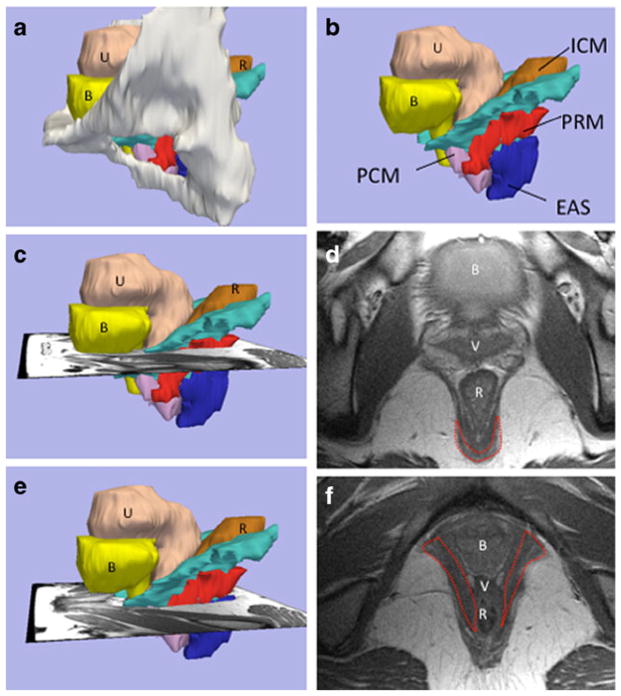
Introduction and hypothesis: The objective of this study was to compare puborectal muscle integrity and bulk in women with both major levator ani (LA) defects on MRI and pelvic organ prolapse (POP) to women with normal LA muscle and normal support.
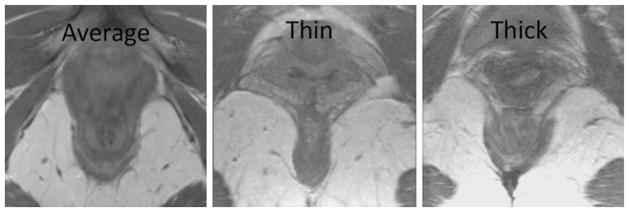
Methods: This is a case-control study comparing 24 cases with known major LA defects and POP to 24 controls with normal LA and normal support. Axial T-2 weighted MRI scans of the pelvis were evaluated for integrity of the puborectal muscle and degree of muscle bulk.
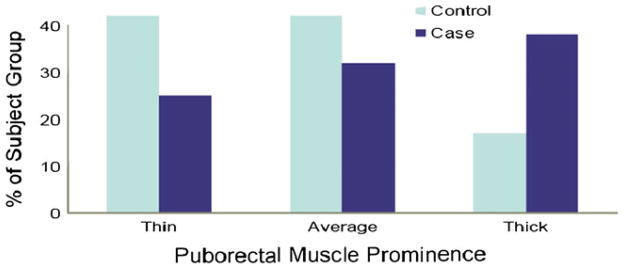
Results: There were no significant group differences in age, body mass index, vaginal deliveries, or hysterectomy status. In all 48 subjects, the puborectal muscle was visible and had no disruption noted. There was no difference in muscle bulk between groups (control/case, thin 42% vs. 25%, average 42% vs. 38%, thick-17% vs. 38%; P = 0.47).
Conclusions: Defects and loss of muscle bulk in the puborectal muscle are not seen on MRI in women with major LA defects and POP.
Conflict of interest statement
Figures
References
-
- Terminologia anatomica=International anatomical terminology. x. Stuttgart: Thieme; 1998. p. 292.
-
- Dietz HP, Lanzarone V. Levator trauma after vaginal delivery. Obstet Gynecol. 2005;106(4):707–712. - PubMed
-
- DeLancey JO, et al. Comparison of levator ani muscle defects and function in women with and without pelvic organ prolapse. Obstet Gynecol. 2007;109(2 Pt 1):295–302. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
