

Deep infiltrating endometriosis of the bowel: MR imaging as a method to predict muscular invasion
- PMID: 21822742
- PMCID: PMC3387499
- DOI: 10.1007/s00261-011-9790-1
Deep infiltrating endometriosis of the bowel: MR imaging as a method to predict muscular invasion
Abstract
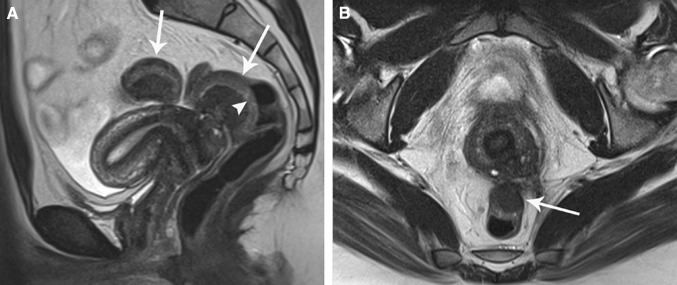
Purpose: To evaluate magnetic resonance (MR) imaging morphologic- and signal intensity abnormalities of deep infiltrating endometriosis (DIE) of the bowel wall and to assess its value in predicting depth and extent of bowel wall infiltration.
Materials and methods: This single-center study was performed in a tertiary referral center for endometriosis. All patients (n = 28) who underwent segmental bowel resection (2004-2010) were retrospectively studied. MR images were analyzed by two experienced readers independently (number of lesions, location, size, signal intensity, and depth of bowel wall infiltration) and this was correlated with histopathology.
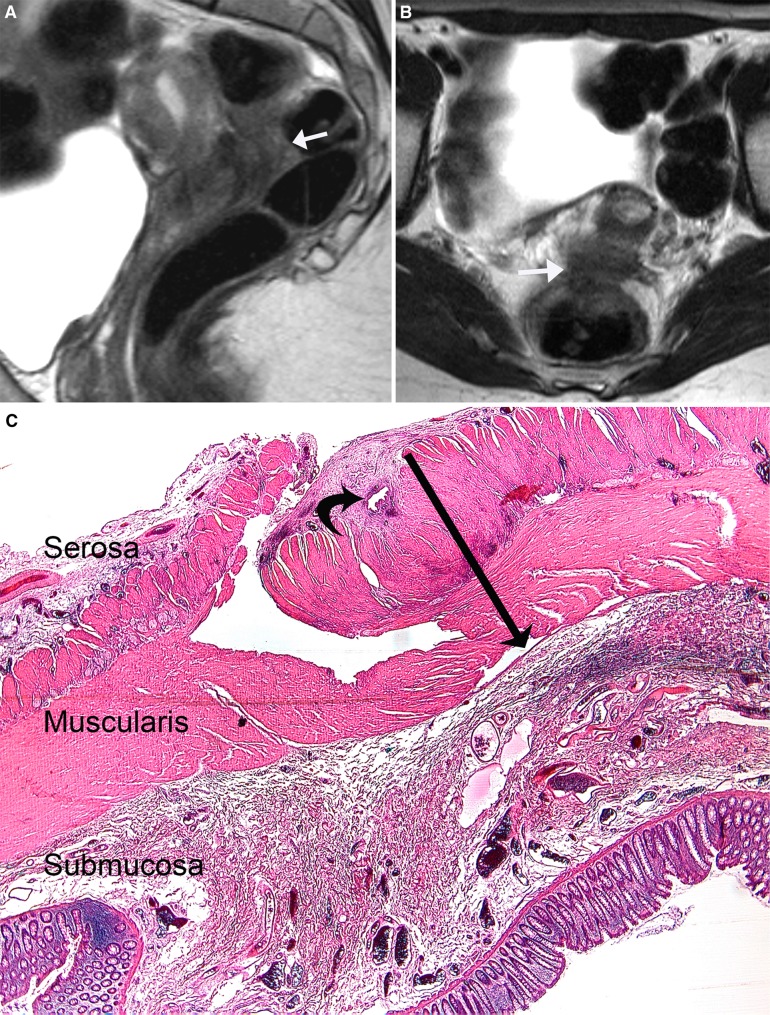
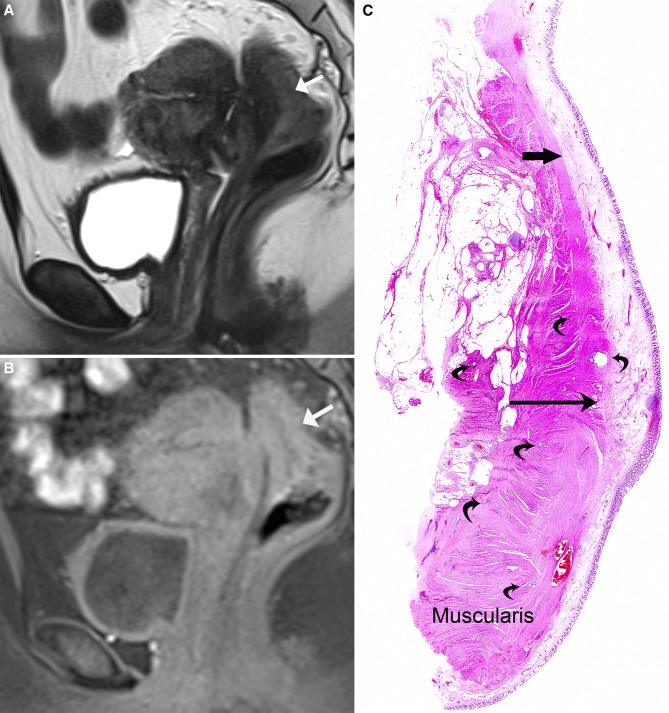
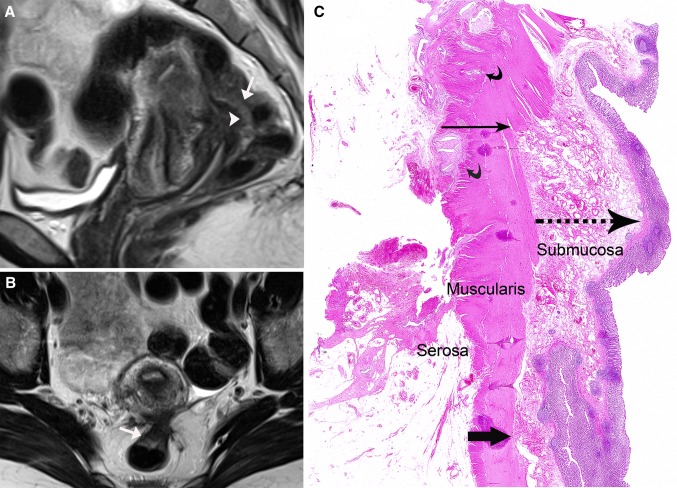
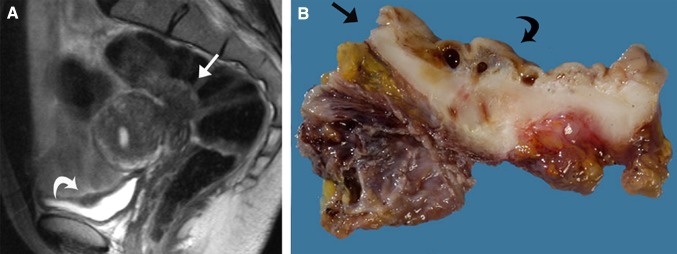
Results: The sensitivity, specificity, positive and negative predictive values, and accuracy for diagnosis of endometriosis infiltrating the muscular layer of the bowel were 100%, 75%, 96%, 100%, and 96%, respectively. The inter-rater agreement was 0.84. "Fan shaped" configurations with hypointensity on T2- and T1-weighted imaging were characteristic for thickening of indigenous smooth muscle and smooth muscle hyperplasia at histopathology, as a consequence of infiltration by endometriosis. Thickening of the (sub)mucosa corresponded to edema with or without infiltration of endometriosis.
Conclusion: MR imaging at 1.5 Tesla is useful to predict muscular infiltration of the bowel in endometriosis, whereas it is of limited value in diagnosis of (sub)mucosal infiltration.
Figures
References
-
- Bazot M, Lafont C, Rouzier R, et al. Diagnostic accuracy of physical examination, transvaginal sonography, rectal endoscopic sonography, and magnetic resonance imaging to diagnose deep infiltrating endometriosis. Fertil Steril. 2009;92(6):1825–1833. doi: 10.1016/j.fertnstert.2008.09.005. - DOI - PubMed
-
- Bazot M, Gasner A, Lafont C, Ballester M, Darai E (2011) Deep pelvic endometriosis: limited additional diagnostic value of postcontrast in comparison with conventional MR images. Eur J Radiol. doi:0.1016/j.ejrad.2010.12.006 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
