

Immunotherapy for prostate cancer: biology and therapeutic approaches
- PMID: 21825260
- PMCID: PMC3675707
- DOI: 10.1200/JCO.2010.34.5025
Immunotherapy for prostate cancer: biology and therapeutic approaches
Abstract
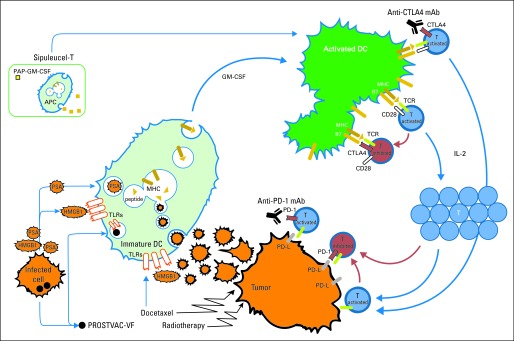
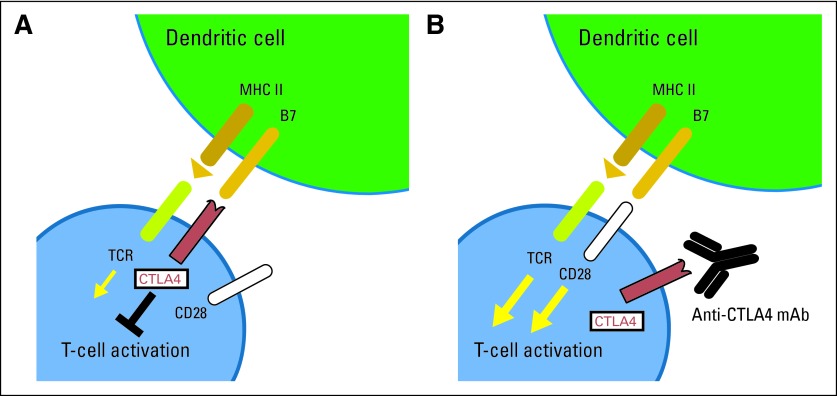
Although prostate cancer was not historically considered to be a particularly immune-responsive cancer, recent clinical trials have demonstrated that immunotherapy for prostate cancer can lead to improvements in overall survival (OS). These studies include randomized controlled trials with sipuleucel-T and another with PROSTVAC-VF, both of which rely on stimulating the immune system to target prostate proteins. This review discusses the most promising developments over the past year in immune-based therapy for prostate cancer and the opportunities that lie ahead. Recent randomized immunotherapy trials in prostate cancer have demonstrated improvements in OS but without the concomitant improvements in progression-free survival. This uncoupling of survival from clinical response poses challenges to clinical management, because conventional measures of objective response cannot be used to identify patients benefiting from treatment. There is a significant need to identify immunologic or clinical surrogates for survival so that clinical benefit can be assessed in a timely manner. Immunotherapy is now an established treatment approach for prostate cancer, with multiple clinical trials demonstrating improvements in OS. Significant challenges to this modality remain, including determining best clinical setting for immunotherapy, identifying patients who benefit, and defining relevant clinical and immunologic end points. Nevertheless, the broader availability of novel immunotherapies will provide opportunities not only to target different components of the immune system but also to combine immunotherapies with other treatments for improved clinical efficacy.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Fong L, Small EJ. Anti-cytotoxic T-lymphocyte antigen-4 antibody: The first in an emerging class of immunomodulatory antibodies for cancer treatment. J Clin Oncol. 2008;26:5275–5283. - PubMed
-
- Brown JA, Dorfman DM, Ma FR, et al. Blockade of programmed death-1 ligands on dendritic cells enhances T cell activation and cytokine production. J Immunol. 2003;170:1257–1266. - PubMed
-
- Fong L, Small EJ. Immunotherapy for prostate cancer. Curr Urol Rep. 2006;7:239–246. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
