

Efficacy of reductive ventricular osmotherapy in a swine model of traumatic brain injury
- PMID: 21826032
- PMCID: PMC3262110
- DOI: 10.1227/NEU.0b013e318230ee5e
Efficacy of reductive ventricular osmotherapy in a swine model of traumatic brain injury
Abstract
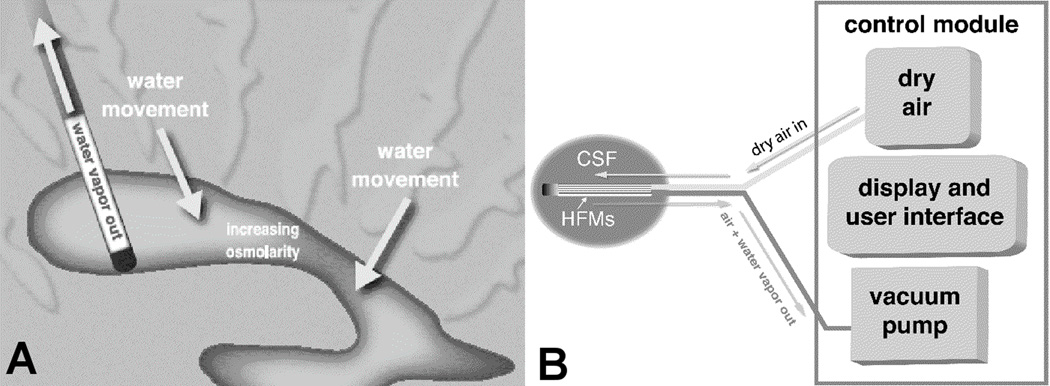
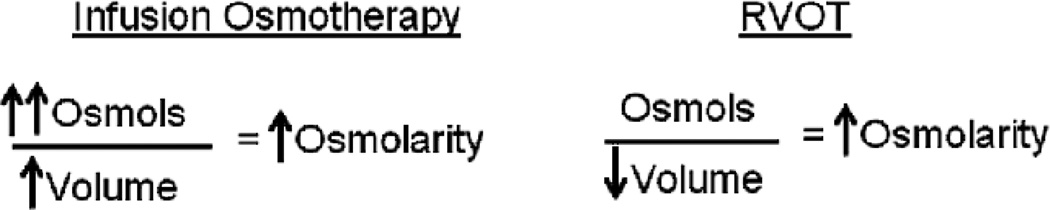
Background: The presence of osmotic gradients in the development of cerebral edema and the effectiveness of osmotherapy are well recognized. A modification of ventriculostomy catheters described in this article provides a method of osmotherapy that is not currently available. The reductive ventricular osmotherapy (RVOT) catheter removes free water from ventricular cerebrospinal fluid (CSF) by incorporating hollow fibers that remove water vapor, thereby providing osmotherapy without increasing osmotic load.
Objective: To increase osmolarity in the ventricular CSF through use of RVOT in vivo.
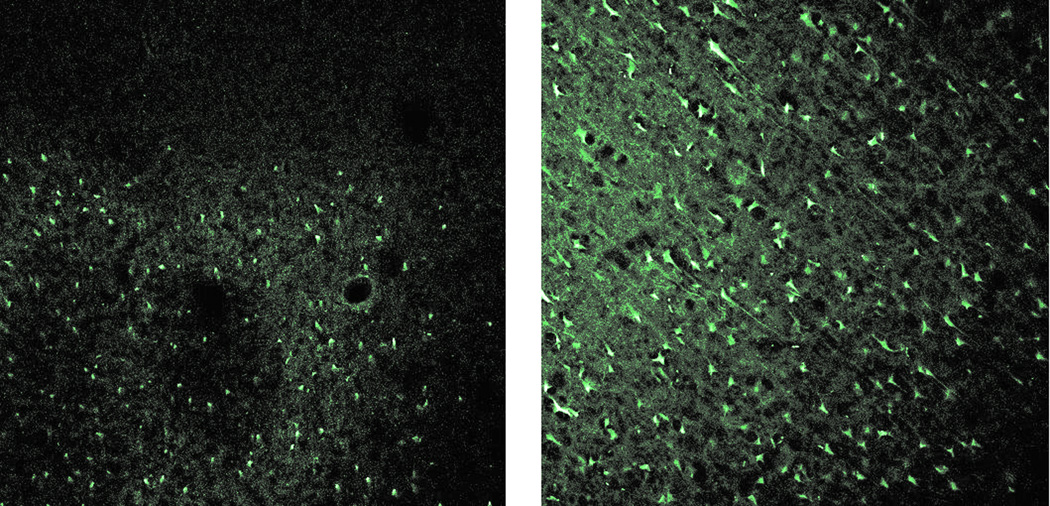
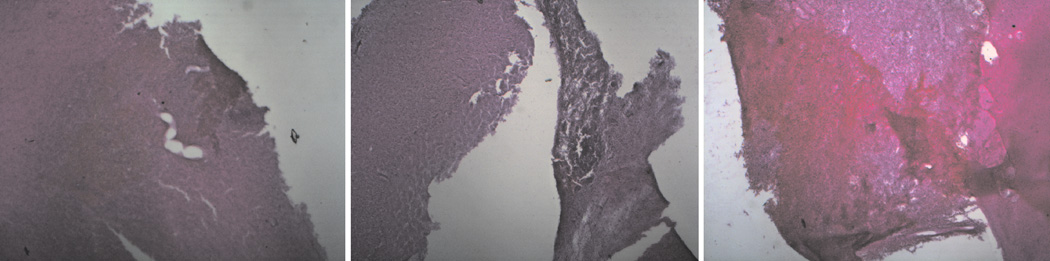
Methods: Twelve Yorkshire swine with contusional injury were randomized to external ventricular drainage (EVD) or RVOT for 12 hours. MR imaging was obtained. Serum, CSF, and brain ultrafiltrate were analyzed. Histology was compared using Fluor-Jade B and hematoxylin and eosin (H & E) stains.
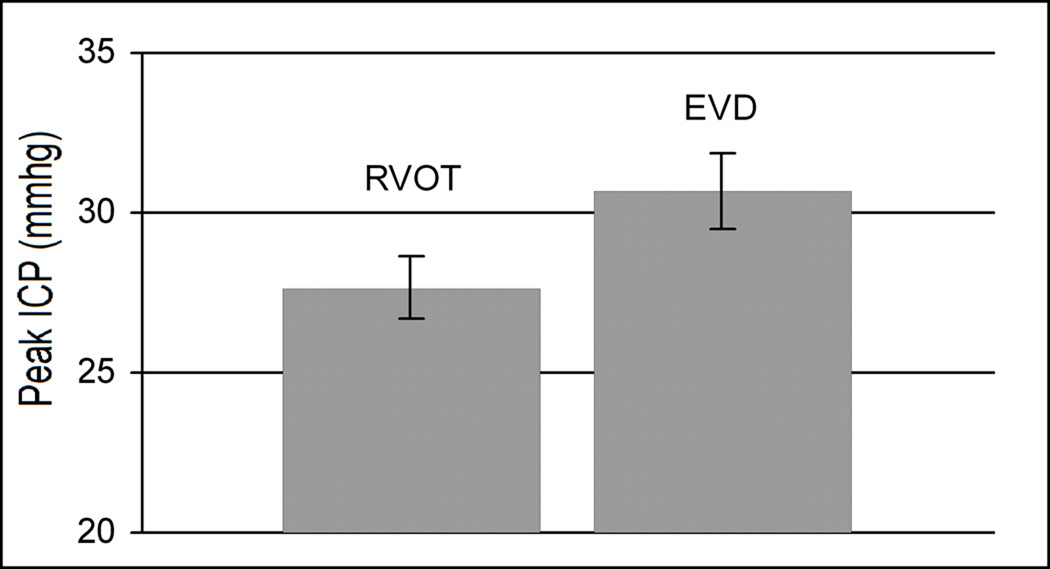
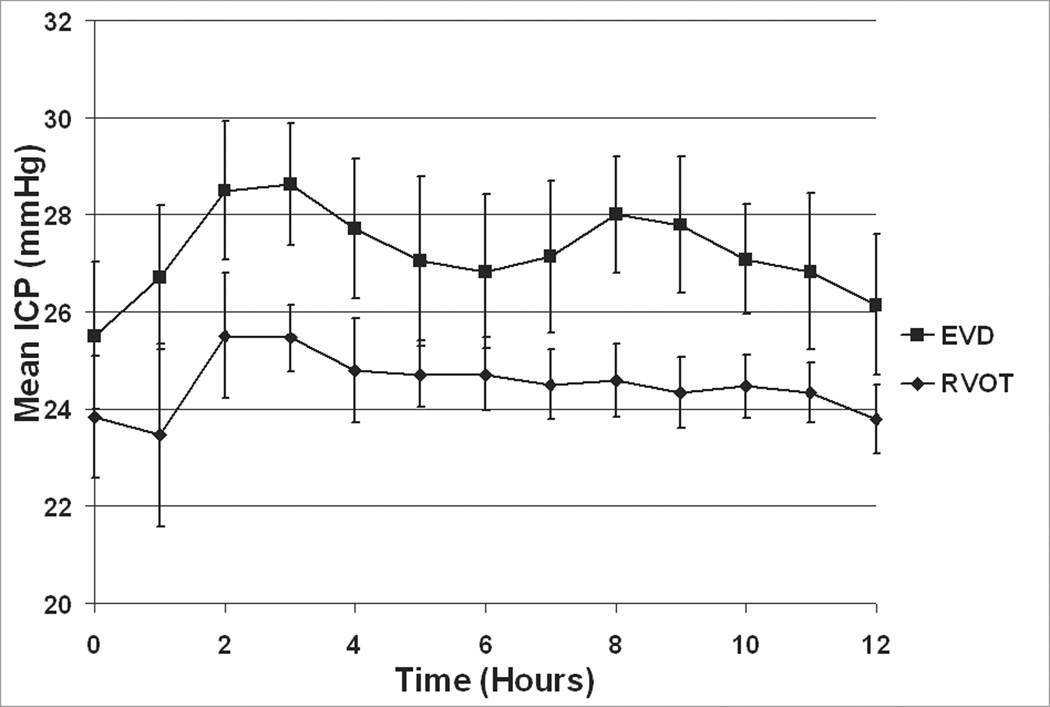
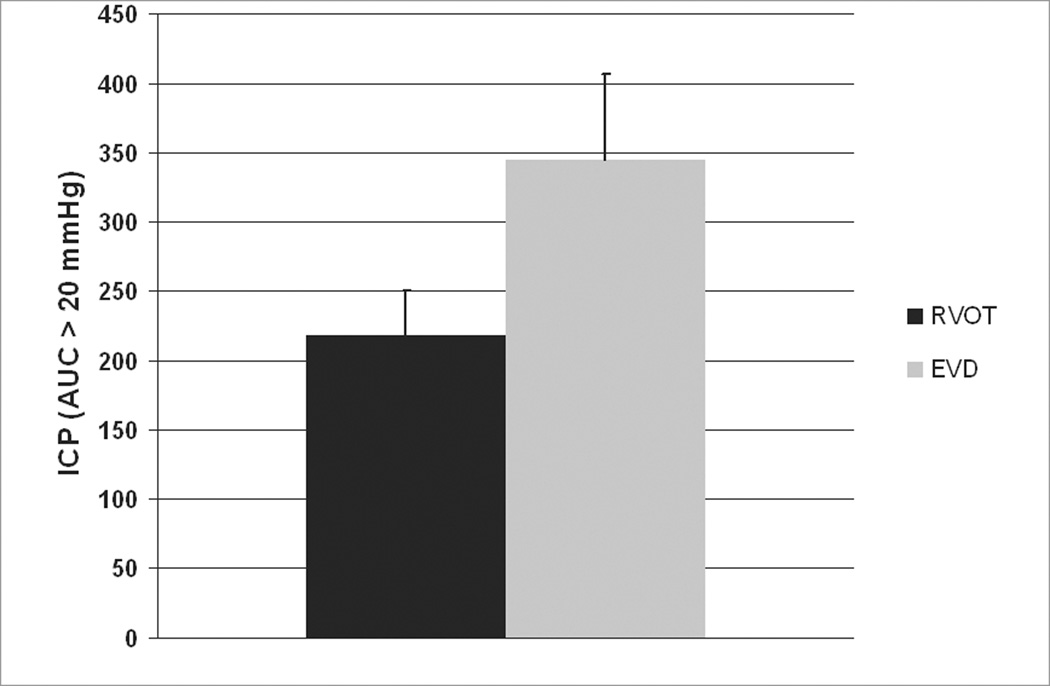
Results: With RVOT, CSF osmolality increased from 292 ± 2.7 to 345 ± 8.0 mOsmol/kg (mean ± SE, P = 0.0006), and the apparent diffusion coefficient (ADC) in the injury region increased from 0.735 ± 0.047 to 1.135 ± .063 (P = 0.004) over 24 hours. With EVD controls, CSF osmolarity and ADC were not significantly changed. Histologically, all RVOT pigs showed no evidence of neuronal degeneration (Grade 1/4) compared to moderate degeneration (Grade 2.6 ± .4/4) seen in EVD treated animals (P = 0.02). The difference in intracranial pressure (ICP) by area under the curve approached significance at P = .065 by Mann Whitney test.
Conclusion: RVOT can increase CSF osmolarity in vivo after experimental traumatic brain injury (TBI). In anticipated clinical use, only a slight increase in CSF osmolarity may be required to reduce cerebral edema.
Figures

References
-
- Marmarou A, Signoretti S, Fatouros PP, Portella G, Aygok GA, Bullock MR. Predominance of cellular edema in traumatic brain swelling in patients with severe head injuries. J Neurosurg. 2006;104:720–730. - PubMed
-
- Bullock MR, Povlishock JT, editors. J Neurotrauma. Vol. 24. 2007. Guidelines for the management of severe traumatic brain injury: 3rd Edition. - PubMed
-
- Vialet R, Albanèse J, Thomachot L, et al. Isovolume hypertonic solutes (sodium chloride or mannitol) in the treatment of refractory posttraumatic intracranial hypertension: 2 mL/kg 7.5% saline is more effective than 2 mL/kg 20% mannitol. Crit Care Med. 2003;31(6):1683–1687. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
