

Medical treatment of benign prostatic hyperplasia
Affiliations
- PMID: 21826125
- PMCID: PMC3151584
Item in Clipboard
Medical treatment of benign prostatic hyperplasia
Rev Urol.
2011.
Abstract
Medical therapy for the treatment of benign prostatic hyperplasia (BPH) became an accepted standard of care in the 1990s following the reports of randomized, double-blind, placebo-controlled studies showing that finasteride, a 5-α reductase inhibitor, and terazosin, an α-blocker, significantly improved lower urinary tract symptoms and increased peak urinary flow rates in men with BPH. This article reviews novel approaches to the pharmacological treatment of BPH.
Keywords: Benign prostatic hyperplasia; Combination therapy; Lower urinary tract symptoms; Monotherapy.
Figures
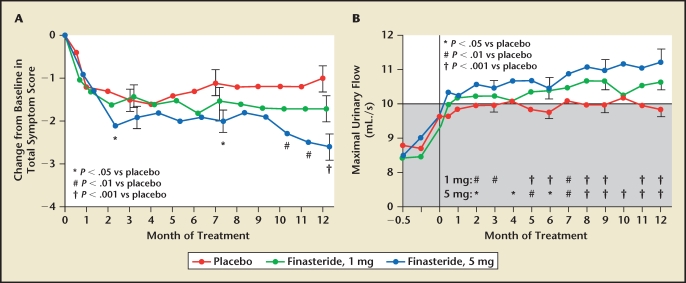
Trial results comparing placebo and two dosing regimens of finasteride in men with benign prostatic hyperplasia. (A) Men who received finasteride, 5 mg, had a significant decrease in symptom scores at months 2, 7, 10, 11, and 12, compared with placebo. Men who received finasteride, 1 mg, had no significant change in symptom scores. (B) At 6 and 12 months, the maximal flow rates in both finasteride-treated groups were significantly higher than baseline values and rates of the placebo group. Shaded area indicates range in which urinary flow was considered to be obstructed. Reproduced with permission from Gormley GJ et al, N Engl J Med. 1992;327:1185–1191. © Massachusetts Medical Society.
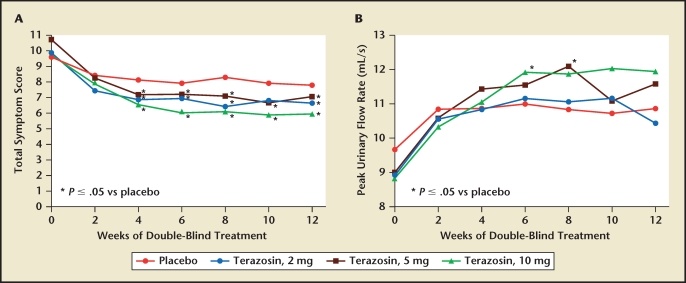
Trial results comparing placebo and three dosing regimens of terazosin in men with benign prostatic hyperplasia. The effects of terazosin on (A) American Urological Association symptom score and (B) peak urinary flow rate were found to be dose dependent. Reproduced with permission from Lepor H et al, J Urol. 1992;148:1467–1474.
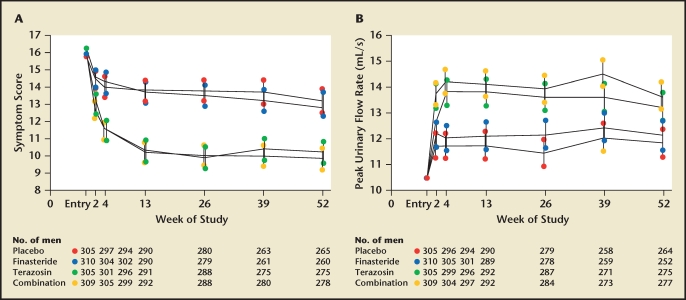
Comparison of finasteride, terazosin, and combined dosing regimens for the treatment of benign prostatic hyperplasia. Symptom scores and flow rates are expressed as adjusted means and 95% confidence intervals. (A) American Urological Association symptom scores, according to treatment group. Symptom scores of subjects who received terazosin or combination therapy were significantly lower from baseline, as well as from those in the placebo and finasteride groups, at all follow-up visits. (B) Mean peak urinary flow rates were significantly higher in the terazosin and combination therapy groups than in the placebo and finasteride groups at all follow-up visits. Reproduced with permission from Lepor H et al, N Engl J Med. 1996;335:533–539. © Massachusetts Medical Society.
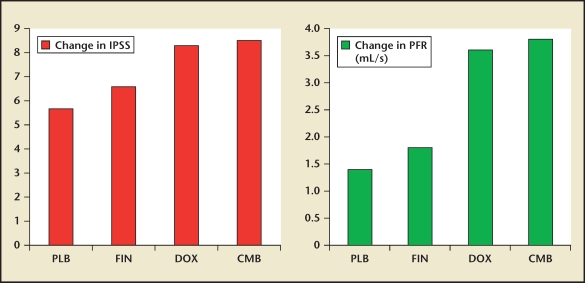
The mean changes in International Prostate Symptom Score (IPSS) score and peak flow rate (PFR) between baseline and 1 year of active treatment of men randomized to placebo (PLB) and finasteride (FIN), doxazosin (DOX), or a finasteride + doxazosin (CMB) in the PREDICT study. Data from Kirby et al.
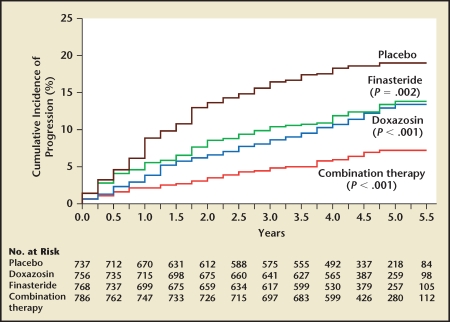
Cumulative incidence of progression of benign prostatic hyperplasia. Progression was defined by an increase of at least 4 points over baseline in the American Urological Association symptom score, acute urinary retention, urinary incontinence, renal insufficiency, or recurrent urinary tract infection. P values are for the comparison with placebo. Reproduced with permission from McConnell JD et al, N Engl J Med. 2003;349:2387–2398. © Massachusetts Medical Society.
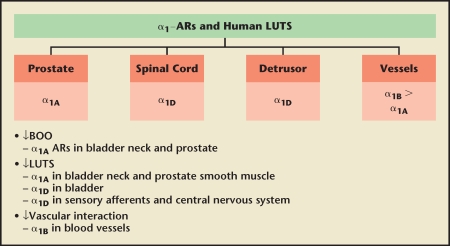
New concepts in drug development of α-blockers. AR, androgen receptor; BOO, bladder outlet obstruction; LUTS, lower urinary tract symptoms. Reproduced with permission from Lepor H, Rev Urol. 2009;11 (suppl 1):S9–S13.
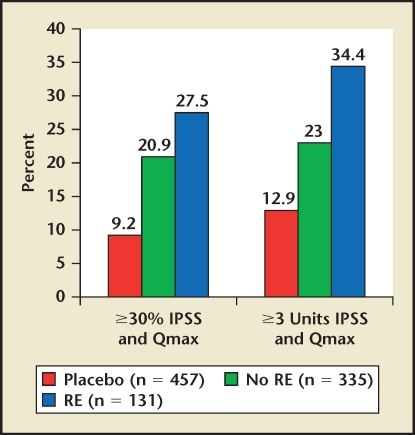
Silodosin post hoc responder analysis by ejaculation status. Based on patient subanalysis. IPSS, International Prostate Symptom Score; RE, retrograde ejaculation. Data on file, Watson Pharmaceuticals, Inc., Corona, CA.
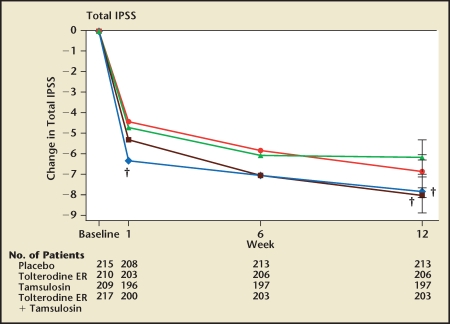
Changes from baseline in International Prostate Symptom Score. Values are adjusted means (ie, leastsquares means). ER, extended release; IPSS, International Prostate Symptom Score. † P < .01 tversus placebo. Reproduced with permission from Kaplan SA et al.
References
-
- Berry SJ, Coffey DS, Walsh PC, Ewing LL. The development of human benign prostatic hyperplasia with age. J Urol. 1984;132:474–479. - PubMed
-
- Shapiro E, Becich MJ, Hartanto V, Lepor H. The relative proportion of stromal and epithelial hyperplasia is related to the development of symptomatic benign prostate hyperplasia. J Urol. 1992;147:1293–1297. - PubMed
-
- Lepor H, Rigaud G. The efficacy of transurethral resection of the prostate in men with moderate symptoms of prostatism. J Urol. 1990;143:533–537. - PubMed
-
- The Finasteride Study Group, authors. Finasteride (MK-906) in the treatment of benign prostatic hyperplasia. Prostate. 1993;22:291–299. - PubMed
-
- Lepor H, Auerbach S, Puras-Baez A, et al. A randomized, placebo-controlled multicenter study of the efficacy and safety of terazosin in the treatment of benign prostatic hyperplasia. J Urol. 1992;148:1467–1474. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources