

A randomized controlled phase Ib trial of the malaria vaccine candidate GMZ2 in African children
- PMID: 21829466
- PMCID: PMC3145647
- DOI: 10.1371/journal.pone.0022525
A randomized controlled phase Ib trial of the malaria vaccine candidate GMZ2 in African children
Abstract
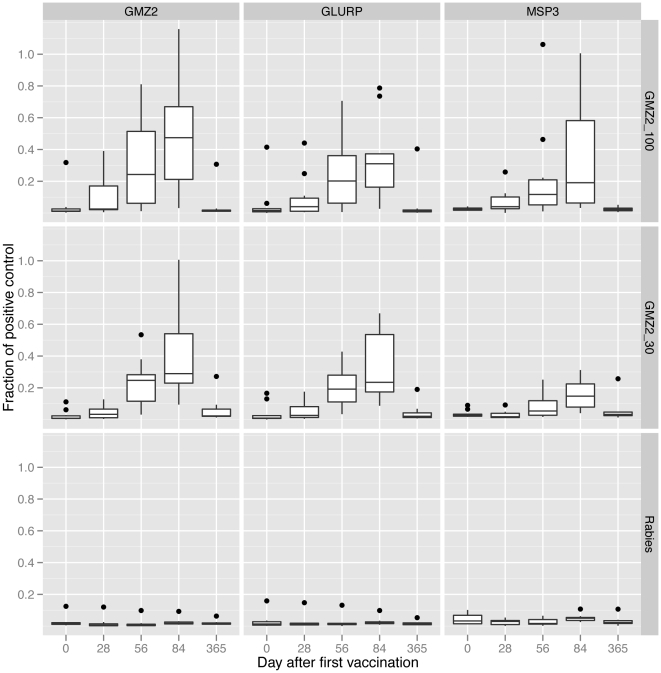
Background: GMZ2 is a fusion protein of Plasmodium falciparum merozoite surface protein 3 (MSP3) and glutamate rich protein (GLURP) that mediates an immune response against the blood stage of the parasite. Two previous phase I clinical trials, one in naïve European adults and one in malaria-exposed Gabonese adults showed that GMZ2 was well tolerated and immunogenic. Here, we present data on safety and immunogenicity of GMZ2 in one to five year old Gabonese children, a target population for future malaria vaccine efficacy trials.
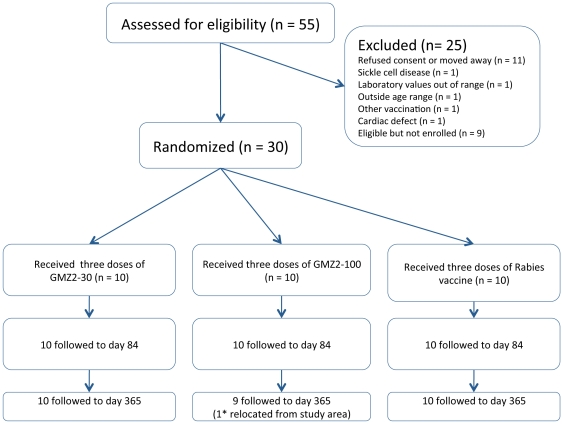
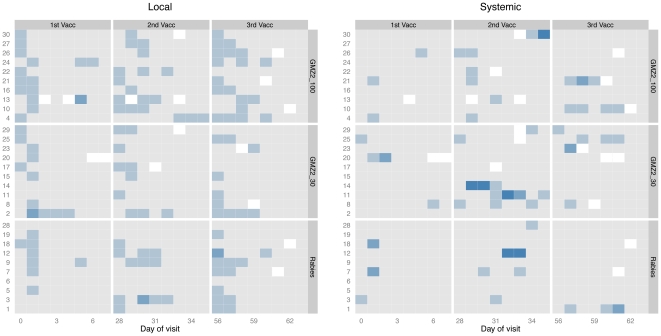
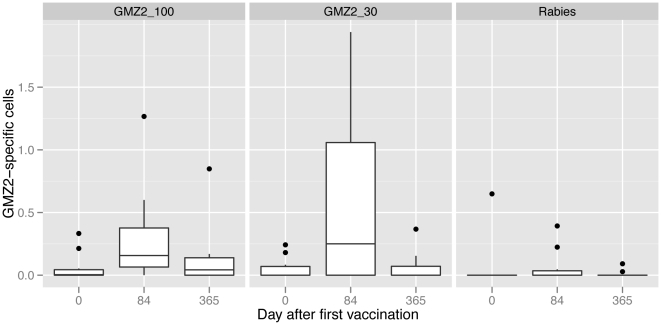
Methodology/principal findings: Thirty children one to five years of age were randomized to receive three doses of either 30 µg or 100 µg of GMZ2, or rabies vaccine. GMZ2, adjuvanted in aluminum hydroxide, was administered on Days 0, 28 and 56. All participants received a full course of their respective vaccination and were followed up for one year. Both 30 µg and 100 µg GMZ2 vaccine doses were well tolerated and induced antibodies and memory B-cells against GMZ2 as well as its antigenic constituents MSP3 and GLURP. After three doses of vaccine, the geometric mean concentration of antibodies to GMZ2 was 19-fold (95%CI: 11,34) higher in the 30 µg GMZ2 group than in the rabies vaccine controls, and 16-fold (7,36) higher in the 100 µg GMZ2 group than the rabies group. Geometric mean concentration of antibodies to MSP3 was 2.7-fold (1.6,4.6) higher in the 30 µg group than in the rabies group and 3.8-fold (1.5,9.6) higher in the 100 µg group. Memory B-cells against GMZ2 developed in both GMZ2 vaccinated groups.
Conclusions/significance: Both 30 µg as well as 100 µg intramuscular GMZ2 are immunogenic, well tolerated, and safe in young, malaria-exposed Gabonese children. This result confirms previous findings in naïve and malaria-exposed adults and supports further clinical development of GMZ2.
Trial registration: ClinicalTrials.gov NCT00703066.
Conflict of interest statement
Figures
References
-
- World Health Organisation. Geneva: WHO; World Malaria Report 2010.
-
- Ballou WR. The development of the RTS,S malaria vaccine candidate: challenges and lessons. Parasite Immunol. 2009;31:492–500. - PubMed
-
- Cohen S, Mc GI, Carrington S. Gamma-globulin and acquired immunity to human malaria. Nature. 1961;192:733–737. - PubMed
-
- Sabchareon A, Burnouf T, Ouattara D, Attanath P, Bouharoun-Tayoun H, et al. Parasitologic and clinical human response to immunoglobulin administration in falciparum malaria. Am J Trop Med Hyg. 1991;45:297–308. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
