

Quantifying the burden and trends of isoniazid resistant tuberculosis, 1994-2009
- PMID: 21829557
- PMCID: PMC3146514
- DOI: 10.1371/journal.pone.0022927
Quantifying the burden and trends of isoniazid resistant tuberculosis, 1994-2009
Abstract
Background: Quantifying isoniazid resistant (INH-R) tuberculosis (TB) is important because isoniazid resistance reduces the probability of treatment success, may facilitate the spread of multidrug resistance, and may reduce the effectiveness of isoniazid preventive therapy (IPT).
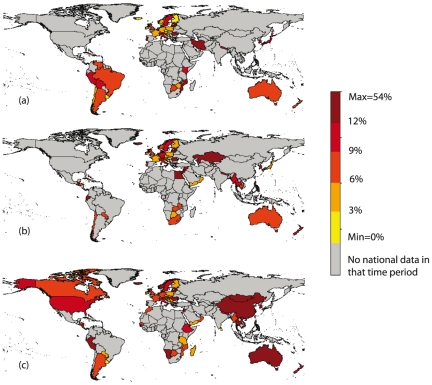
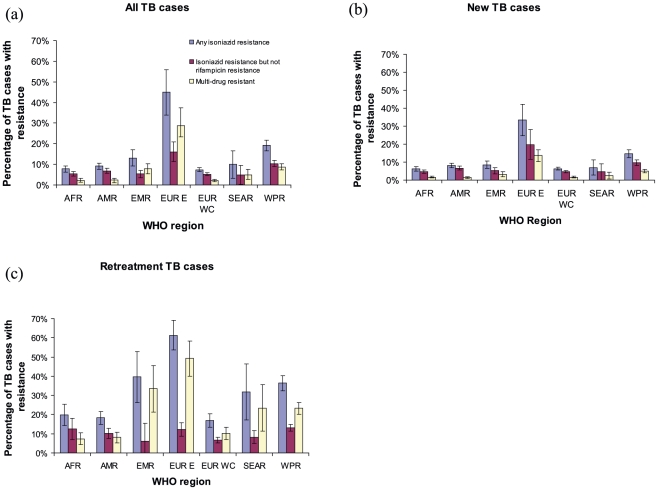
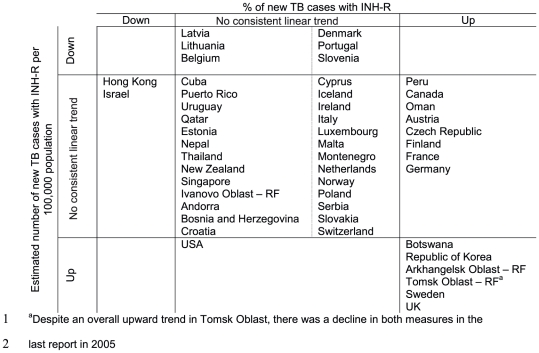
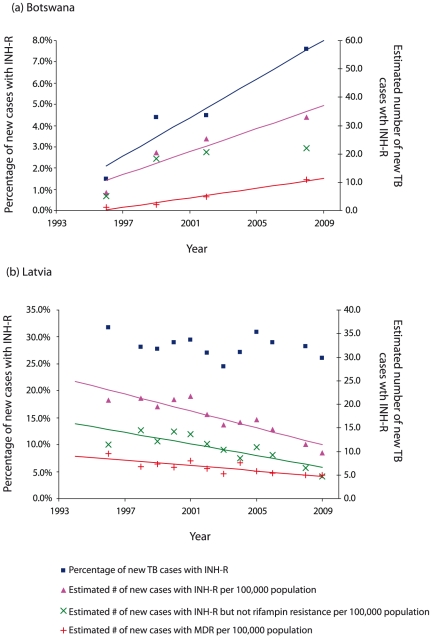
Methodology/principal findings: We used data reported to the World Health Organization between 1994-2009 to estimate the INH-R burden among new and retreatment TB cases. We assessed geographical and temporal variation in INH-R and reported levels in high HIV prevalence countries (≥2%) to understand implications for IPT. 131 settings reported INH-R data since 1994. A single global estimate of the percentage of incident TB cases with INH-R was deemed inappropriate due to particularly high levels in the Eastern European region where 44.9% (95% CI: 34.0%, 55.8%) of incident TB cases had INH-R. In all other regions combined, 13.9% (95% CI: 12.6%, 15.2%) of incident cases had INH-R with the lowest regional levels seen in West/Central Europe and Africa. Where trend data existed, we found examples of rising and falling burdens of INH-R. 40% of high HIV prevalence countries reported national data on INH-R and 7.3% (95% CI: 5.5%, 9.1%) of cases in these settings had INH-R.
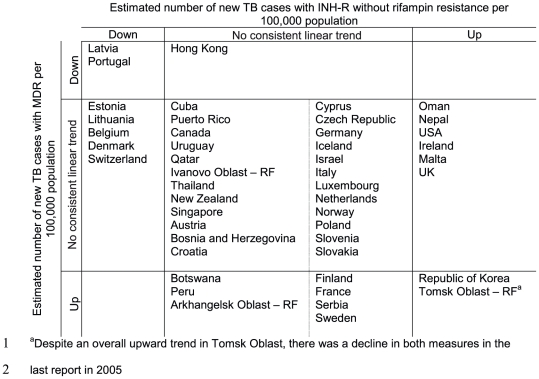
Conclusions/significance: Outside the Eastern European region, one in seven incident TB cases has INH-R, while this rises to nearly half within Eastern Europe. Many countries cannot assess trends in INH-R and the scarcity of data from high HIV prevalence areas limits insight into the implications for IPT. Further research is required to understand reasons for the observed time trends and to determine the effects of INH-R for control of TB.
Conflict of interest statement
Figures
References
-
- World Health Organization. Geneva: Stop TB Department. WHO Press; 2010. Global Tuberculosis Control 2010. WHO/HTM/TB/2010. 7. Available: http://whqlibdoc.who.int/publications/2010/9789241564069_eng.pdf. ISBN: 978 92 4 156406 9.
-
- World Health Organization. Geneva: WHO Press; 2010. Multidrug and extensively drug-resistant (M/XDR-TB). 2010 Global Report on Surveillance and Response. WHO/HTM/TB/2010. 3. Available: http://whqlibdoc.who.int/publications/2010/9789241599191_eng.pdf. ISBN: 978 92 4 159919 1.
-
- Sirgel FA, Donald PR, Odhiambo J, Githui W, Umapathy KC, et al. A multicentre study of the early bactericidal activity of anti-tuberculosis drugs. J Antimicrob Chemother. 2000;45:859–870. - PubMed
-
- Hafner R, Cohn JA, Wright DJ, Dunlap NE, Egorin MJ, et al. Early bactericidal activity of isoniazid in pulmonary tuberculosis. Optimization of methodology. The DATRI 008 Study Group. Am J Respir Crit Care Med. 1997;156:918–923. - PubMed
-
- Rieder H. Paris: International Union Against Tuberculosis and Lung Disease; 2002. Interventions for Tuberculosis Control and Elimination.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
