

Levothyroxine monotherapy cannot guarantee euthyroidism in all athyreotic patients
- PMID: 21829633
- PMCID: PMC3148220
- DOI: 10.1371/journal.pone.0022552
Levothyroxine monotherapy cannot guarantee euthyroidism in all athyreotic patients
Abstract
Context: Levothyroxine monotherapy is the treatment of choice for hypothyroid patients because peripheral T4 to T3 conversion is believed to account for the overall tissue requirement for thyroid hormones. However, there are indirect evidences that this may not be the case in all patients.
Objective: To evaluate in a large series of athyreotic patients whether levothyroxine monotherapy can normalize serum thyroid hormones and thyroid-pituitary feedback.
Design: Retrospective study.
Setting: Academic hospital.
Patients: 1,811 athyreotic patients with normal TSH levels under levothyroxine monotherapy and 3,875 euthyroid controls.
Measurements: TSH, FT4 and FT3 concentrations by immunoassays.
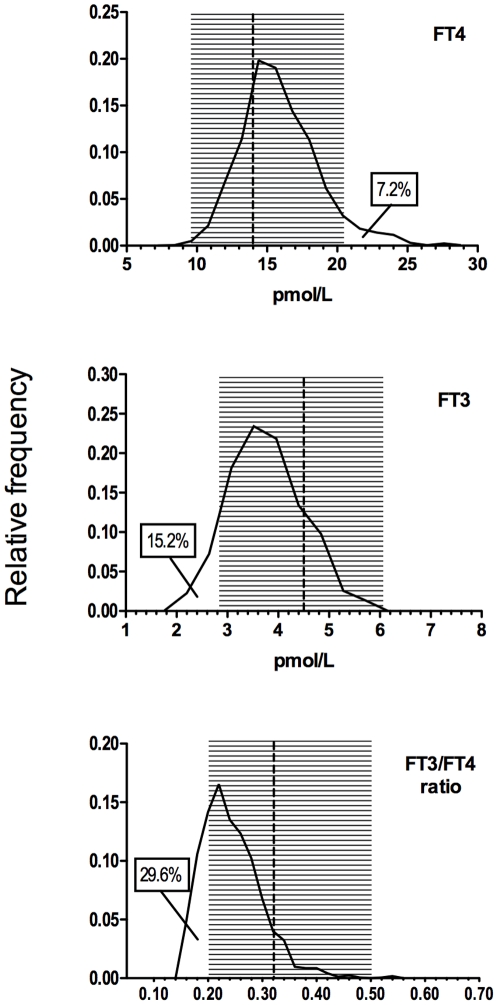
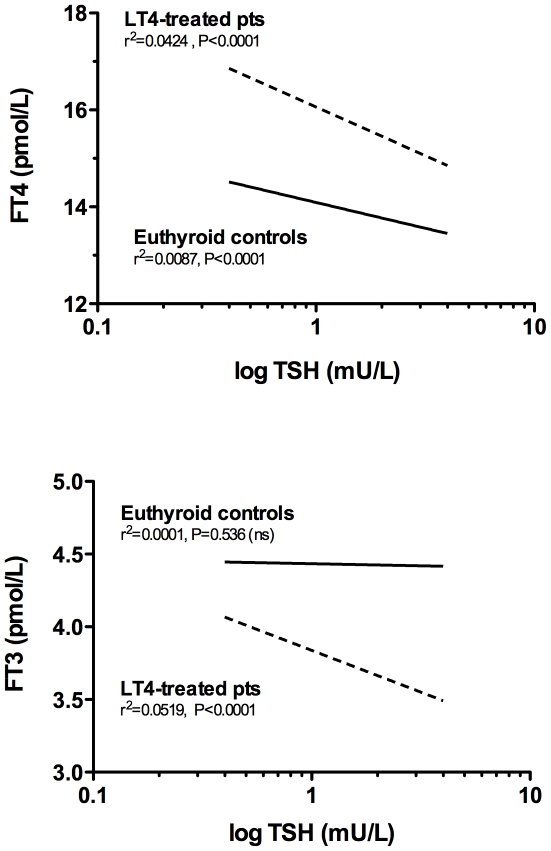
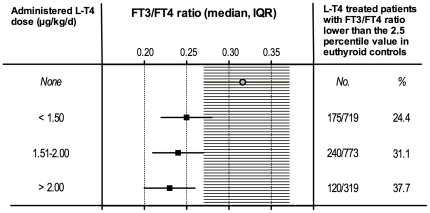
Results: FT4 levels were significantly higher and FT3 levels were significantly lower (p<0.001 in both cases) in levothyroxine-treated athyreotic patients than in matched euthyroid controls. Among the levothyroxine-treated patients 15.2% had lower serum FT3 and 7.2% had higher serum FT4 compared to euthyroid controls. A wide range of FT3/FT4 ratios indicated a major heterogeneity in the peripheral T3 production capacity in different individuals. The correlation between thyroid hormones and serum TSH levels indicated an abnormal feedback mechanism in levothyroxine-treated patients.
Conclusions: Athyreotic patients have a highly heterogeneous T3 production capacity from orally administered levothyroxine. More than 20% of these patients, despite normal TSH levels, do not maintain FT3 or FT4 values in the reference range, reflecting the inadequacy of peripheral deiodination to compensate for the absent T3 secretion. The long-term effects of chronic tissue exposure to abnormal T3/T4 ratio are unknown but a sensitive marker of target organ response to thyroid hormones (serum TSH) suggests that this condition causes an abnormal pituitary response. A more physiological treatment than levothyroxine monotherapy may be required in some hypothyroid patients.
Conflict of interest statement
Figures
References
-
- Bunevicius R, Kazanavicius G, Zalinkevicius R, Prange AJ., Jr Effects of thyroxine as compared with thyroxine plus triiodothyronine in patients with hypothyroidism. N Engl J Med. 1999;340:424–9. - PubMed
-
- Appelhof BC, Fliers E, Wekking EM, Schene AH, Huyser J, et al. Combined therapy with levothyroxine and liothyronine in two ratios, compared with levothyroxine monotherapy in primary hypothyroidism: a double-blind, randomized, controlled clinical trial. J Clin Endocrinol Metab. 2005;90:2666–74. - PubMed
-
- Woeber KA. Levothyroxine therapy and serum free thyroxine and free triiodothyronine concentrations. J Endocrinol Invest. 2002;25:106–9. - PubMed
-
- Iverson JF, Mariash CN. Optimal free thyroxine levels for thyroid hormone replacement in hypothyroidism. Endocr Pract. 2008;14:550–5. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
