

Secondary Buruli ulcer skin lesions emerging several months after completion of chemotherapy: paradoxical reaction or evidence for immune protection?
- PMID: 21829740
- PMCID: PMC3149035
- DOI: 10.1371/journal.pntd.0001252
Secondary Buruli ulcer skin lesions emerging several months after completion of chemotherapy: paradoxical reaction or evidence for immune protection?
Abstract
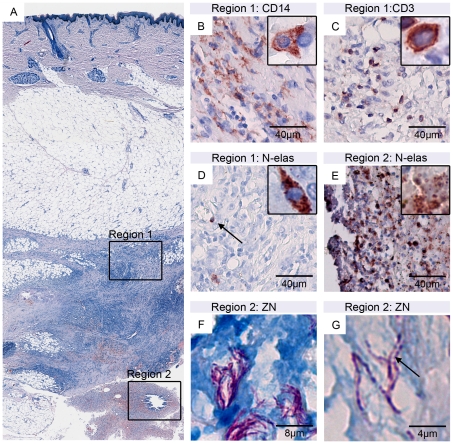
Background: The neglected tropical disease Buruli ulcer (BU) caused by Mycobacterium ulcerans is an infection of the subcutaneous tissue leading to chronic ulcerative skin lesions. Histopathological features are progressive tissue necrosis, extracellular clusters of acid fast bacilli (AFB) and poor inflammatory responses at the site of infection. After the recommended eight weeks standard treatment with rifampicin and streptomycin, a reversal of the local immunosuppression caused by the macrolide toxin mycolactone of M. ulcerans is observed.
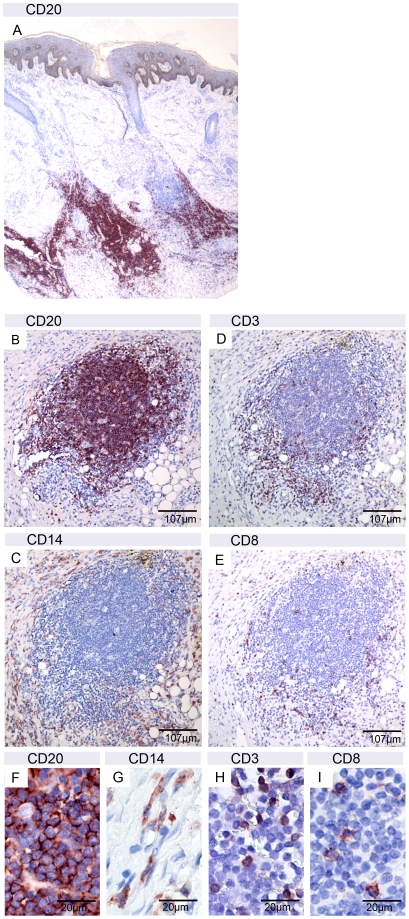
Methodology/principal findings: We have conducted a detailed histopathological and immunohistochemical analysis of tissue specimens from two patients developing multiple new skin lesions 12 to 409 days after completion of antibiotic treatment. Lesions exhibited characteristic histopathological hallmarks of Buruli ulcer and AFB with degenerated appearance were found in several of them. However, other than in active disease, lesions contained massive leukocyte infiltrates including large B-cell clusters, as typically found in cured lesions.
Conclusion/significance: Our histopathological findings demonstrate that the skin lesions emerging several months after completion of antibiotic treatment were associated with M. ulcerans infection. During antibiotic therapy of Buruli ulcer development of new skin lesions may be caused by immune response-mediated paradoxical reactions. These seem to be triggered by mycobacterial antigens and immunostimulators released from clinically unrecognized bacterial foci. However, in particular the lesions that appeared more than one year after completion of antibiotic treatment may have been associated with new infection foci resolved by immune responses primed by the successful treatment of the initial lesion.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


References
-
- Evans MR, Thangaraj HS, Wansbrough-Jones MH. Buruli ulcer. Curr Opin Infect Dis. 2000;13:109–112. - PubMed
-
- Johnson PDR, Stinear T, Small PLC, Pluschke G, Merritt RW, et al. Buruli ulcer (M. ulcerans infection): new insights, new hope for disease control. PLoS Med. 2005;2:e108. doi: 10.1371/journal.pmed.0020108. - DOI - PMC - PubMed
-
- Walsh DS, Portaels F, Meyers WM. Buruli ulcer (Mycobacterium ulcerans infection). Trans R Soc Trop Med Hyg. 2008;102:969–978. doi: 10.1016/j.trstmh.2008.06.006. - DOI - PubMed
-
- Asiedu K, Scherpbier, R, Raviglione, M . Geneva: World Health Organization; 2000. Buruli ulcer: Mycobacterium ulcerans infection.
-
- Rondini S, Horsfield C, Mensah-Quainoo E, Junghanss T, Lucas S, et al. Contiguous spread of Mycobacterium ulcerans in Buruli ulcer lesions analysed by histopathology and real-time PCR quantification of mycobacterial DNA. The Journal of Pathology. 2006;208:119–128. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
