

Sagittal balance analysis after pedicle subtraction osteotomy in ankylosing spondylitis
- PMID: 21830080
- PMCID: PMC3175913
- DOI: 10.1007/s00586-011-1929-9
Sagittal balance analysis after pedicle subtraction osteotomy in ankylosing spondylitis
Abstract
Introduction: This is a radiographic study of ankylosing spondylitis patients with severe fixed kyphotic deformity who underwent pedicle subtraction osteotomy. Our goal was to measure and validate new angle to assess global kyphosis and to evaluate the sagittal balance after surgery. This is the first report which describes new angle to assess global kyphosis (T1-S1).
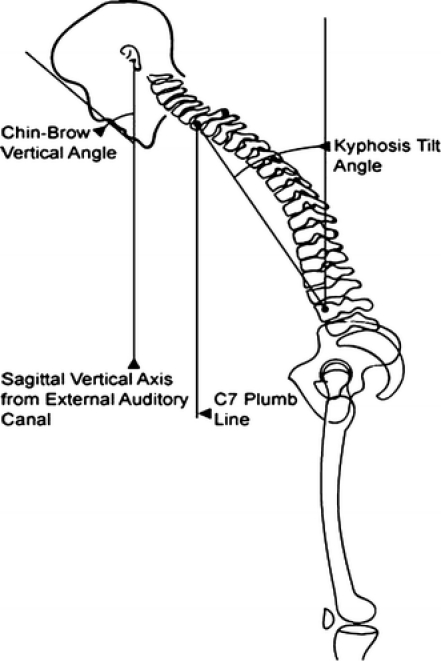
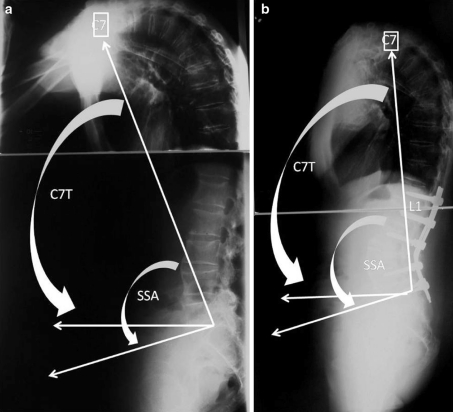
Materials and methods: Pre and postoperative controls were compared according to the Pelvic Incidence. The sagittal parameters ankylosing spondylitis patients were compared with 154 asymptomatic patients. In addition to the pelvic parameters and the C7 tilt, we used the spino-sacral angle.
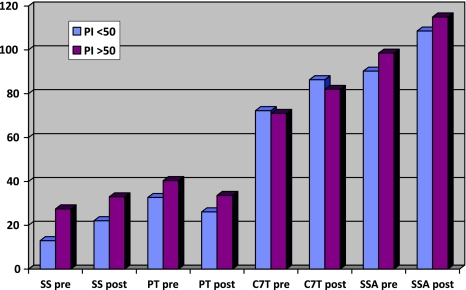
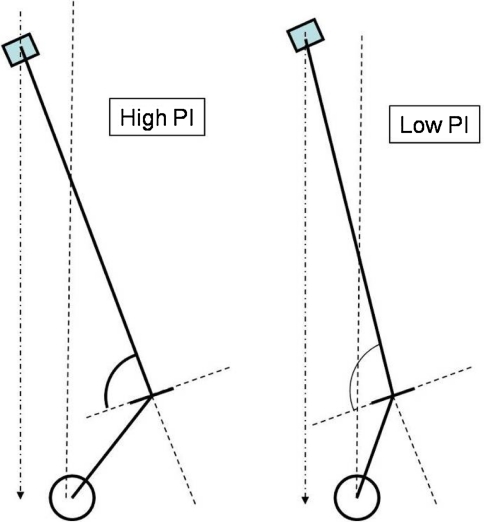
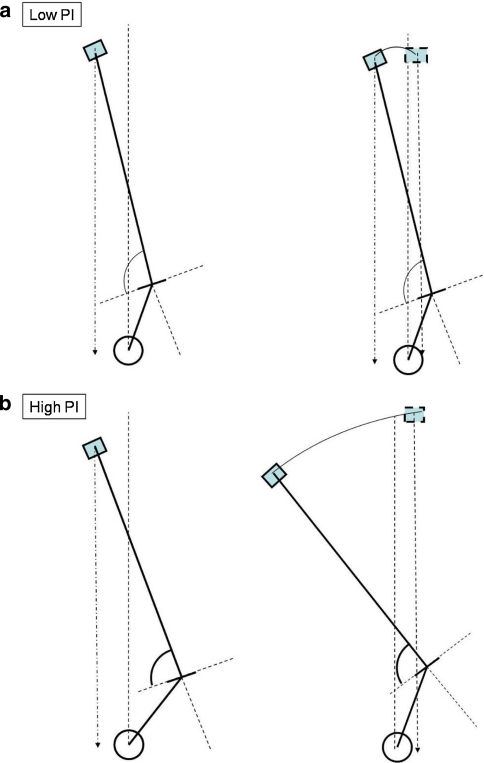
Results: Pelvic incidence in ankylosing spondylitis patients was higher than asymptomatic population (61° vs. 51°). For a same tilt of C7 for both groups, the low pelvic incidence group had a lower sacral slope and pelvic tilt and a higher global kyphosis (spino-sacral angle = 90°) than the high pelvic incidence group (spino-sacral angle = 98°). In the adult volunteers, the C7 tilt and spino-sacral angle measured, respectively, 95° and 135°. The preoperative C7 tilt measured 73° and increased to 83° (p = 0.0025). The preoperative spino-sacral angle measured 96° and increased to 113.3° (p = 0.003).
Conclusion: A low pelvic incidence pelvis has a lower sacral slope than in high pelvic incidence and can support a bigger kyphosis. All the parameters were improved by the pedicle subtraction osteotomy, but the average spinosacral angle remained lower than the control group. When C7 tilt was useful to assess the improvement of the sagittal balance, SSA allowed a better evaluation of the correction of kyphosis itself.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
