

Recurrent, sequential, bilateral deep cerebellar hemorrhages: a case report
- PMID: 21831285
- PMCID: PMC3177913
- DOI: 10.1186/1752-1947-5-360
Recurrent, sequential, bilateral deep cerebellar hemorrhages: a case report
Abstract
Introduction: Hypertensive intra-cerebral hemorrhage is usually a one-time event and recurrences are rare. Most recurrences develop as part of long-term failure of blood pressure control. The site of the re-bleed is usually limited to the basal ganglia and thalami.
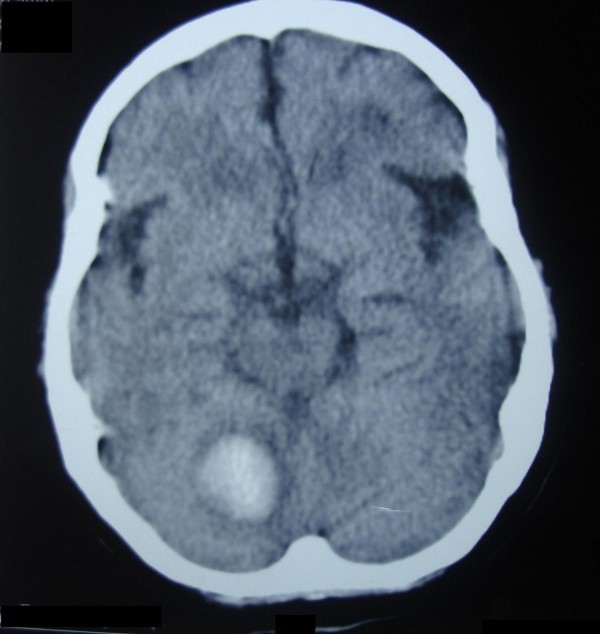
Case presentation: We report the case of a 59-year-old hypertensive Caucasian woman who developed two sequential, right- and then left-sided, deep cerebellar hemorrhages. The second hemorrhage followed the first one by 57 days, at a time when her blood pressure was optimally controlled. In spite of these critical sites and short duration between the two bleeds, the patient achieved a relatively good functional recovery. Her brain magnetic resonance angiogram was unremarkable.
Conclusion: The development of recurrent hypertensive hemorrhage is rare and usually occurs within two years of the first bleed. To the best of our knowledge, this is the first reported case of bilateral, sequential, right- and then left-sided deep cerebellar hemorrhages. These hemorrhages were separated by eight weeks and the patient had a relatively good functional recovery. We believe that hypertension was the etiology behind these hemorrhages.
Figures

References
-
- Mohr JP, Caplan LR, Melski JW, Goldstein RJ, Duncan GW, Kistler JP, Pessin MS, Bleich HL. The Harvard Cooperative Stroke Registry: A prospective registry. Neurology. 1978;28:754–763. - PubMed
-
- Adams HP, Jr, Biller J. In: Clinical Neurology. Joynt RJ, Griggs RC, editor. Vol. 2. Philadelphia: Lippincott-Raven Publishers; 1993. Hemorrhagic intracranial vascular disease; pp. 1–49.
-
- Biller J, Shah MV. In: Conn's Current Therapy. Rakel RE, editor. Philadelphia: WB Saunders; 1997. Intracerebral hemorrhage; pp. 877–880.
-
- Thrift AG, McNeil JJ, Forbes A, Donnan GA. Three important subgroups of hypertensive persons at greater risk of intracerebral hemorrhage. Melbourne Risk Factor Study Group. Hypertension. 1998;31:1223–1229. - PubMed
LinkOut - more resources
Full Text Sources
