

Dosing regimens of oral ciprofloxacin for children with severe malnutrition: a population pharmacokinetic study with Monte Carlo simulation
- PMID: 21831986
- PMCID: PMC3172043
- DOI: 10.1093/jac/dkr314
Dosing regimens of oral ciprofloxacin for children with severe malnutrition: a population pharmacokinetic study with Monte Carlo simulation
Abstract
Background: Severe malnutrition is frequently complicated by sepsis, leading to high case fatality. Oral ciprofloxacin is a potential alternative to the standard parenteral ampicillin/gentamicin combination, but its pharmacokinetics in malnourished children is unknown.
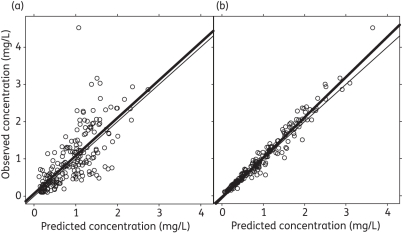
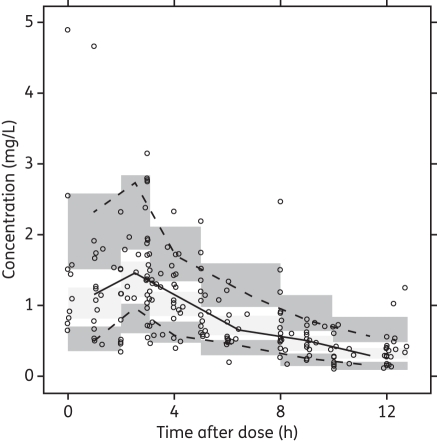
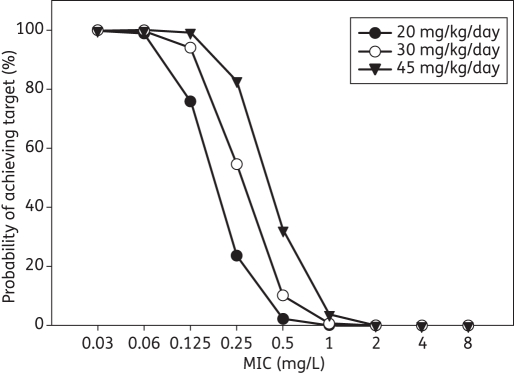
Methods: Ciprofloxacin (10 mg/kg, 12 hourly) was administered either 2 h before or up to 2 h after feeds to Kenyan children hospitalized with severe malnutrition. Four plasma ciprofloxacin concentrations were measured over 24 h. Population analysis with NONMEM investigated factors affecting the oral clearance (CL) and the oral volume of distribution (V). Monte Carlo simulations investigated dosage regimens to achieve a target AUC(0-24)/MIC ratio of ≥125.
Results: Data comprised 202 ciprofloxacin concentration measurements from 52 children aged 8-102 months. Absorption was generally rapid but variable; C(max) ranged from 0.6 to 4.5 mg/L. Data were fitted by a one-compartment model with first-order absorption and lag. The parameters were CL (L/h) = 42.7 (L/h/70 kg) × [weight (kg)/70](0.75) × [1 + 0.0368 (Na(+) - 136)] × [1 - 0.283 (high risk)] and V (L) = 372 × (L/70 kg) × [1 + 0.0291 (Na(+) - 136)]. Estimates of AUC(0-24) ranged from 8 to 61 mg·h/L. The breakpoint for Gram-negative organisms was <0.06 mg/L with doses of 20 mg/kg/day and <0.125 mg/L with doses of 30 or 45 mg/kg/day. The cumulative fraction of response with 30 mg/kg/day was ≥80% for Escherichia coli, Klebsiella pneumoniae and Salmonella species, but <60% for Pseudomonas aeruginosa.
Conclusions: An oral ciprofloxacin dose of 10 mg/kg three times daily (30 mg/kg/day) may be a suitable alternative antibiotic for the management of sepsis in severely malnourished children. Absorption was unaffected by the simultaneous administration of feeds.
Figures

References
-
- Ashworth A, Chopra M, McCoy D, et al. WHO guidelines for management of severe malnutrition in rural South African hospitals: effect on case fatality and the influence of operational factors. Lancet. 2004;363:1110–5. doi:10.1016/S0140-6736(04)15894-7. - DOI - PubMed
-
- Maitland K, Berkley JA, Shebbe M, et al. Children with severe malnutrition: can those at highest risk of death be identified with the WHO protocol? PLoS Medicine. 2006;3:e500. doi:10.1371/journal.pmed.0030500. - DOI - PMC - PubMed
-
- Bachou H, Tylleskär T, Kaddu-Mulindwa DH, et al. Bacteraemia among severely malnourished children infected and uninfected with the human immunodeficiency virus-1 in Kampala, Uganda. BMC Infect Dis. 2006;6:160. doi:10.1186/1471-2334-6-160. - DOI - PMC - PubMed
