

Chronic kidney disease worsens sepsis and sepsis-induced acute kidney injury by releasing High Mobility Group Box Protein-1
- PMID: 21832986
- PMCID: PMC3491658
- DOI: 10.1038/ki.2011.261
Chronic kidney disease worsens sepsis and sepsis-induced acute kidney injury by releasing High Mobility Group Box Protein-1
Abstract
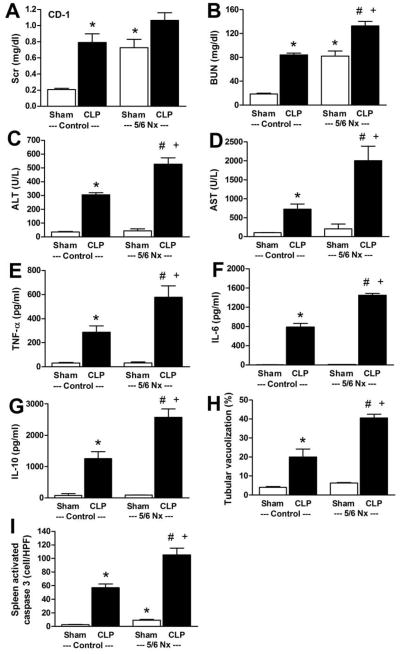
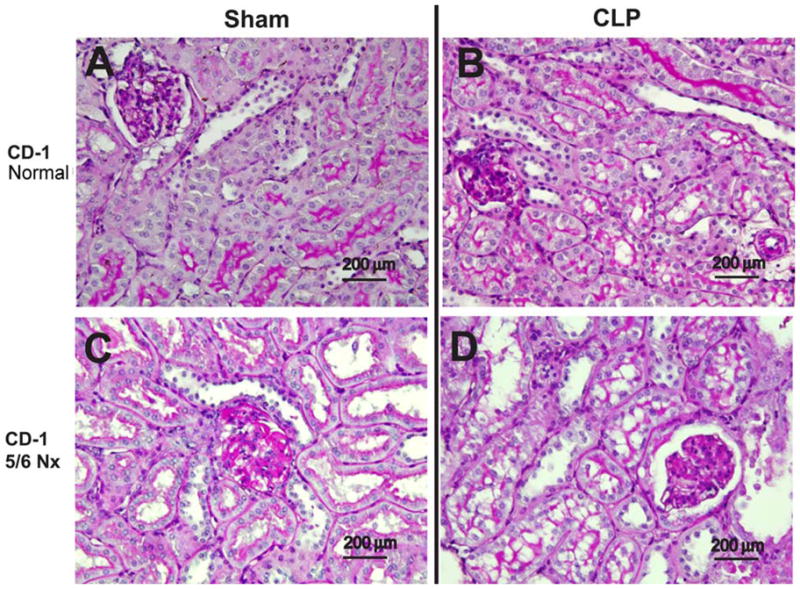
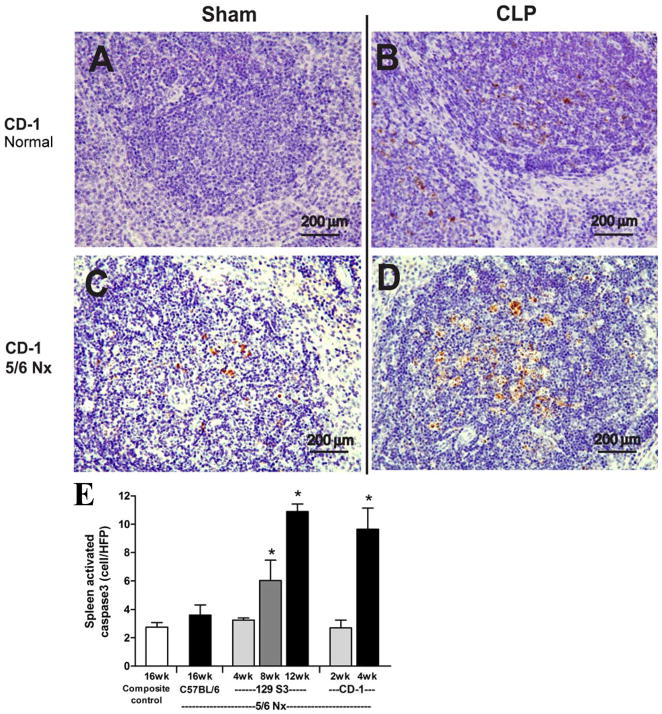
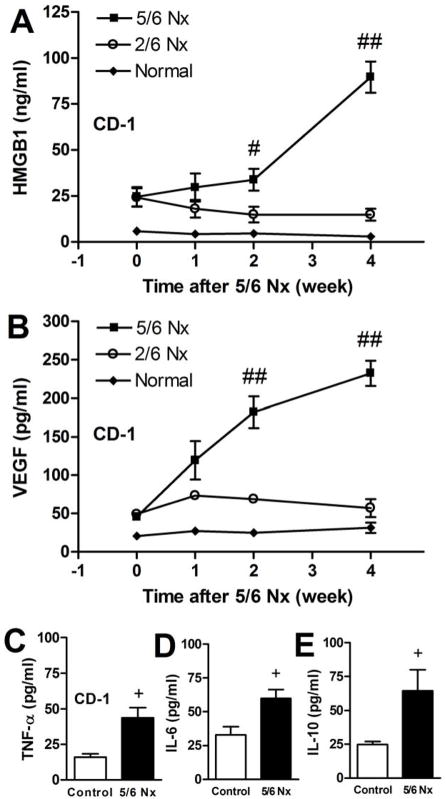
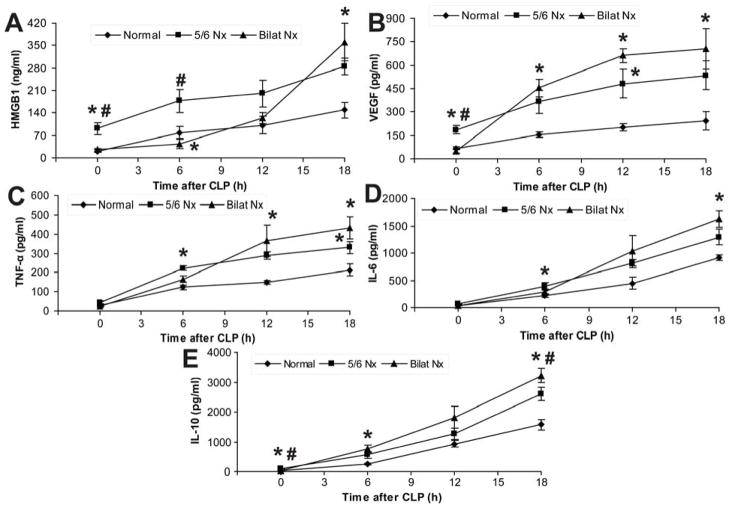
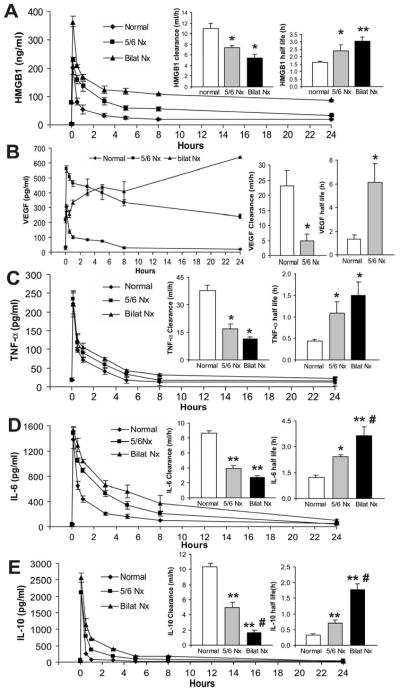
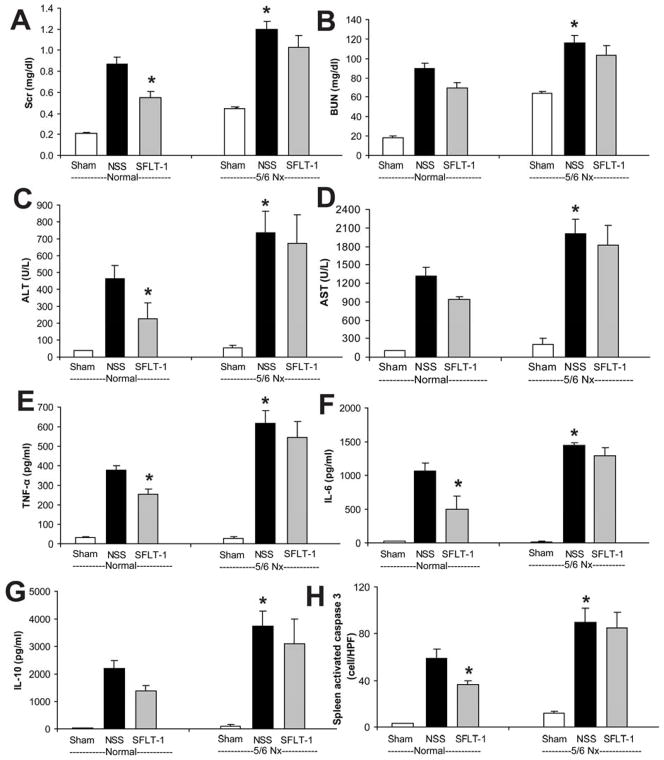
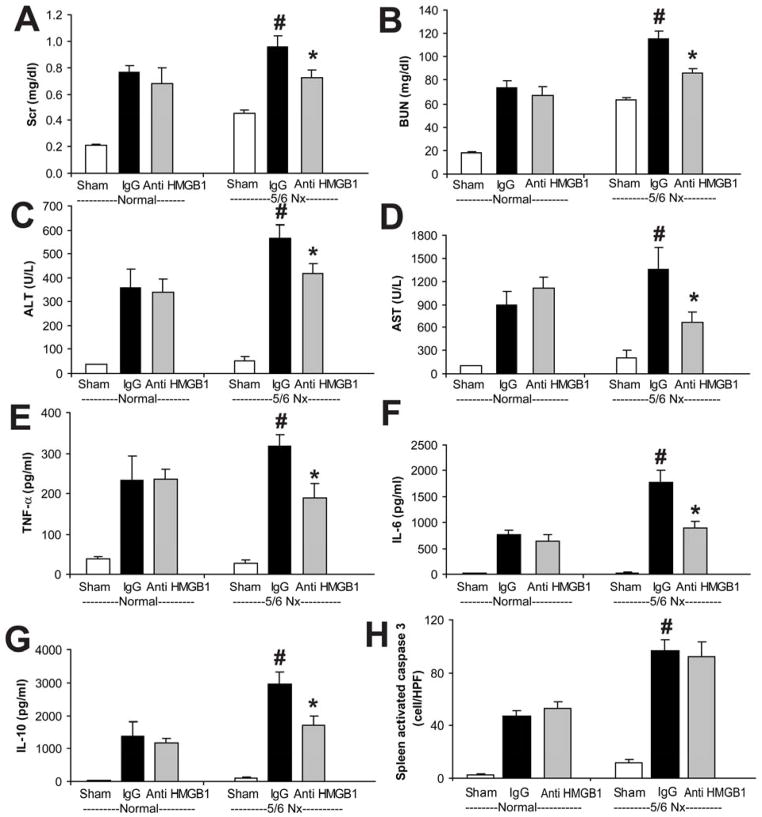
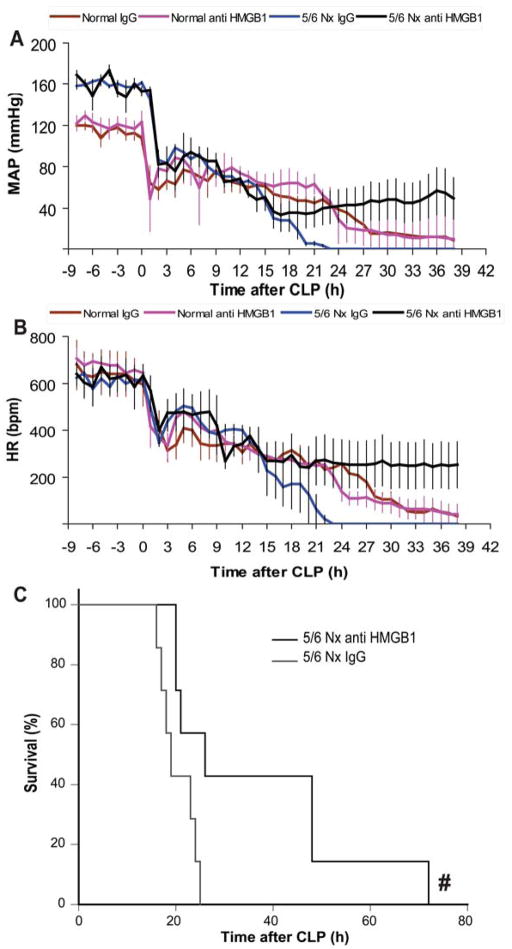
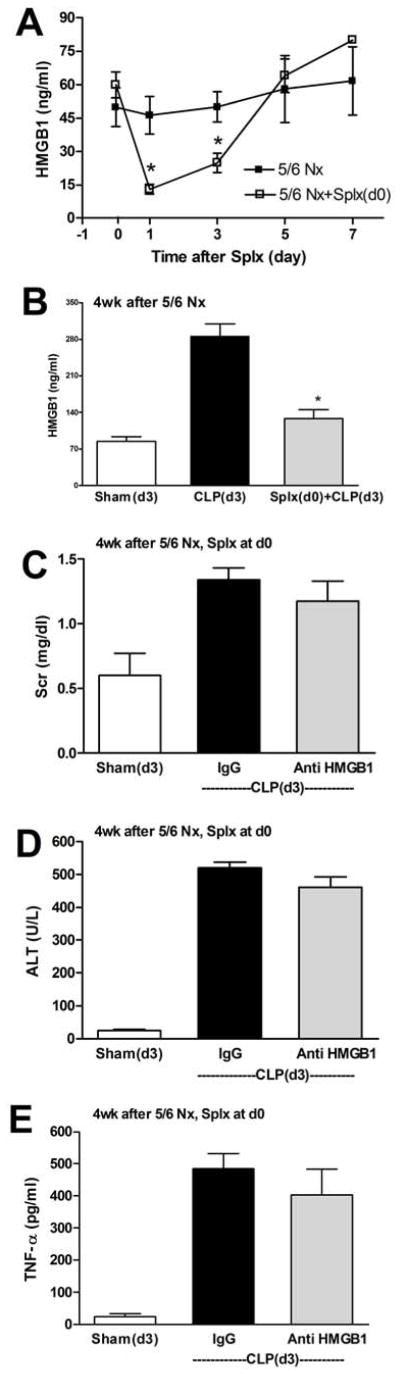
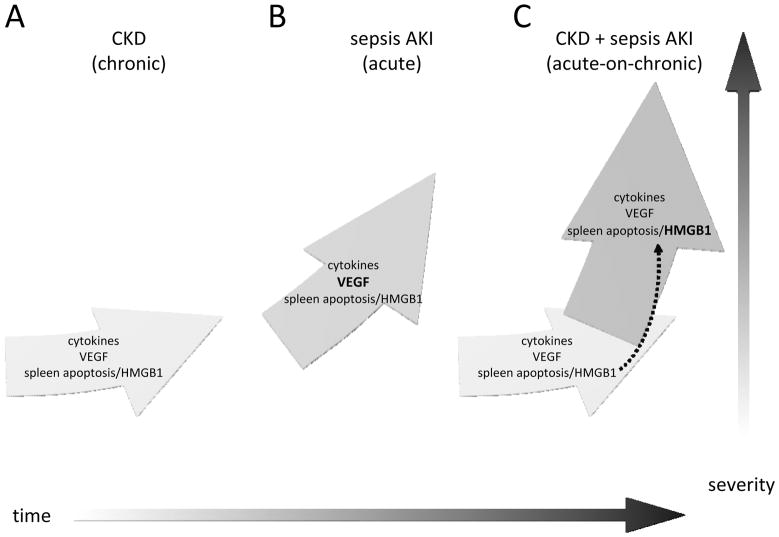
We have shown that folate-induced kidney dysfunction and interstitial fibrosis predisposes mice to sepsis mortality. Agents that increase survival in normal septic mice were ineffective in a two-stage kidney disease model. Here we used the 5/6 nephrectomy mouse model of progressive chronic kidney disease (CKD) to study how CKD affects acute kidney injury (AKI) induced by sepsis. We induced sepsis using cecal ligation and puncture and found that the presence of CKD intensified the severity of kidney and liver injury, cytokine release, and splenic apoptosis. Accumulation of High Mobility Group Box Protein-1 (HMGB1; a late proinflammatory cytokine released from apoptotic cells), vascular endothelial growth factor (VEGF), tumor necrosis factor (TNF)-α, interleukin (IL)-6, or IL-10 was increased in CKD or sepsis alone and to a greater extent in CKD-sepsis. Only part of the increase was explained by decreased renal clearance. Surprisingly, we found splenic apoptosis in CKD, even in the absence of sepsis. Although VEGF neutralization with soluble fms-like tyrosine kinase 1 (sFLT-1) (a soluble VEGF receptor) effectively treated sepsis, it was ineffective against CKD-sepsis. A single dose of HMGB1-neutralizing antiserum administered 6 h after sepsis alone was ineffective; however, CKD-sepsis was attenuated by anti-HMGB1. Splenectomy transiently decreased circulating HMGB1 levels, reversing the effectiveness of anti-HMGB1 treatment on CKD-sepsis. Thus, progressive CKD increases the severity of sepsis, in part, by reducing the renal clearance of several cytokines. CKD-induced splenic apoptosis and HMGB1 release could be important common mediators for both CKD and sepsis.
Figures
References
-
- Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med. 2003 Apr 17;348(16):1546–54. - PubMed
-
- Dyson A, Singer M. Animal models of sepsis: why does preclinical efficacy fail to translate to the clinical setting? Crit Care Med. 2009 Jan;37(1 Suppl):S30–7. - PubMed
-
- Esmon CT. Why do animal models (sometimes) fail to mimic human sepsis? Crit Care Med. 2004 May;32(5 Suppl):S219–22. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
