

Pharmacogenetics in the brazilian population
- PMID: 21833165
- PMCID: PMC3153000
- DOI: 10.3389/fphar.2010.00118
Pharmacogenetics in the brazilian population
Abstract
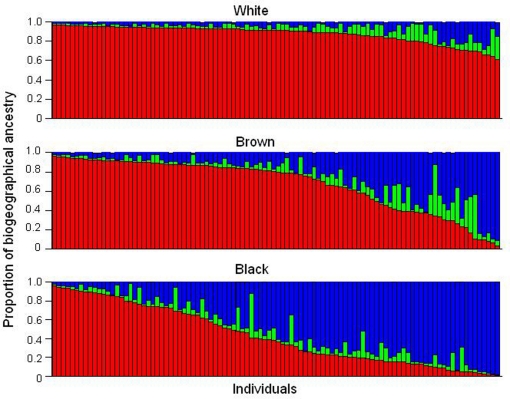
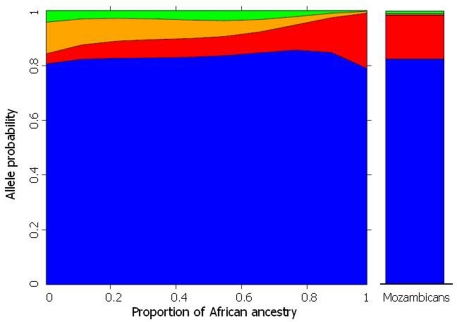
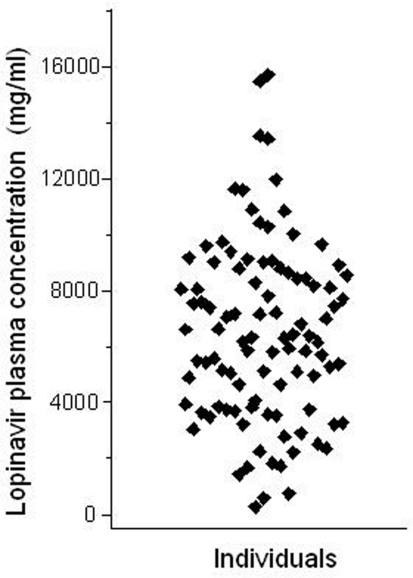
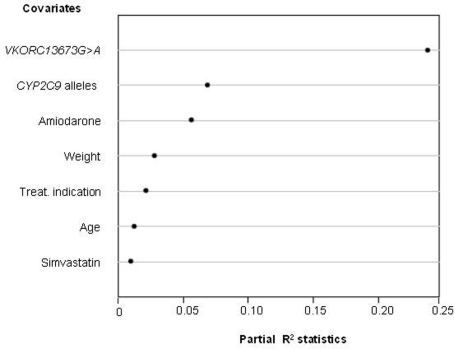
Brazil is the fifth largest country in the world and its present population, in excess of 190;million, is highly heterogeneous, as a result of centuries of admixture between Amerindians, Europeans, and Sub-Saharan Africans. The estimated individual proportions of biogeographical ancestry vary widely and continuously among Brazilians: most individuals, irrespective of self-identification as White, Brown or Black - the major categories of the Brazilian Census "race/color" system - have significant degrees of European and African ancestry, while a sizeable number display also Amerindian ancestry. These features have important pharmacogenetic (PGx) implications: first, extrapolation of PGx data from relatively well-defined ethnic groups is clearly not applicable to the majority of Brazilians; second, the frequency distribution of polymorphisms in pharmacogenes (e.g., CYP3A5, CYP2C9, GSTM1, ABCB1, GSTM3, VKORC, etc) varies continuously among Brazilians and is not captured by race/color self-identification; third, the intrinsic heterogeneity of the Brazilian population must be acknowledged in the design and interpretation of PGx studies in order to avoid spurious conclusions based on improper matching of study cohorts. The peculiarities of PGx in Brazilians are illustrated with data for different therapeutic groups, such as anticoagulants, HIV protease inhibitors and non-steroidal antinflammatory drugs, and the challenges and advantages created by population admixture for the study and implementation of PGx are discussed. PGx data for Amerindian groups and Brazilian-born, first-generation Japanese are presented to illustrate the rich diversity of the Brazilian population. Finally, I introduce the reader to the Brazilian Pharmacogenetic Network or Refargen, a nation-wide consortium of research groups, with the mission to provide leadership in PGx research and education in Brazil, with a population health impact.
Keywords: Brazilian pharmacogenetic network; HIV protease inhibitors; biogeographical ancestry; non-steroidal anti-inflammatory drugs; population admixture; warfarin.
Figures
References
-
- Estrela R. C. E., Ribeiro F. S., Barroso P. F., Tuyama M., Gregório S. P., Dias-Neto E., Struchiner C. J., Suarez-Kurtz G. (2009). ABCB1 polymorphisms have no impact on the concentrations of lopinavir and ritonavir in blood, semen and saliva of HIV-infected men under stable antiretroviral therapy. Pharmacogenomics 10, 311–31810.2217/14622416.10.2.311 - DOI - PubMed
-
- Gage B. F., Eby C., Johnson J. A., Deych E., Rieder M. J., Ridker P. M., Milligan P. E., Grice G., Lenzini P., Rettie A. E., Aquilante C. L., Grosso L., Marsh S., Langaee T., Farnett L. E., Voora D., Veenstra D. L., Glynn R. J., Barrett A., McLeod H. L. (2008). Use of pharmacogenetic and clinical factors to predict the therapeutic dose of warfarin. Clin. Pharmacol. Ther. 84, 326–33110.1038/clpt.2008.10 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous