

Differentiation of pancreatic cysts with optical coherence tomography (OCT) imaging: an ex vivo pilot study
- PMID: 21833374
- PMCID: PMC3149535
- DOI: 10.1364/BOE.2.002372
Differentiation of pancreatic cysts with optical coherence tomography (OCT) imaging: an ex vivo pilot study
Abstract
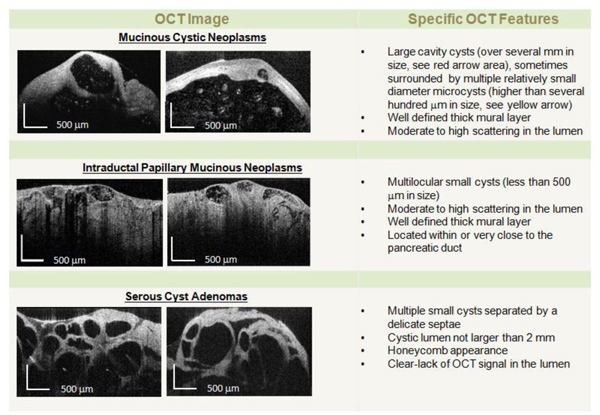
We demonstrate for the first time that optical coherence tomography (OCT) imaging can reliably distinguish between morphologic features of low risk pancreatic cysts (i.e., pseudocysts and serous cystadenomas) and high risk pancreatic cysts (i.e., mucinous cystic neoplasms and intraductal papillary mucinous neoplasms). In our study fresh pancreatectomy specimens (66) from patients with cystic lesions undergoing surgery were acquired and examined with OCT. A training set of 20 pathology-OCT correlated tissue specimens were used to develop criteria for differentiating between low and high risk cystic lesions. A separate (validation) set of 46 specimens were used to test the OCT criteria by three clinicians, blinded to histopathology findings. Histology was finally used as a 'gold' standard for testing OCT findings. OCT was able to reveal specific morphologic features of pancreatic cysts and thus to differentiate between low-risk and high-risk cysts with over 95% sensitivity and specificity. This pilot study suggests that OCT could be used by clinicians in the future to more reliably differentiate between benign and potentially malignant pancreatic cysts. However, in vivo use of OCT requires a probe that has to fit the bore of the pancreas biopsy needle. Therefore, we have developed such probes and planned to start an in vivo pilot study within the very near future.
Keywords: (170.0170) Medical optics and biotechnology; (170.4500) Optical coherence tomography; (170.4580) Optical diagnostics for medicine; (170.6935) Tissue characterization.
Figures



References
LinkOut - more resources
Full Text Sources
Other Literature Sources