

Rapid complete reversal of systemic hypoperfusion after intra-aortic balloon pump counterpulsation and survival in cardiogenic shock complicating an acute myocardial infarction
- PMID: 21835287
- PMCID: PMC3155687
- DOI: 10.1016/j.ahj.2011.04.025
Rapid complete reversal of systemic hypoperfusion after intra-aortic balloon pump counterpulsation and survival in cardiogenic shock complicating an acute myocardial infarction
Abstract
Background: In patients with cardiogenic shock (CS) complicating an acute myocardial infarction, a strategy of early revascularization (ERV) versus initial medical stabilization (IMS) improves survival. Intra-aortic balloon counterpulsation (IABC) provides hemodynamic support and facilitates coronary angiography and revascularization in CS patients.
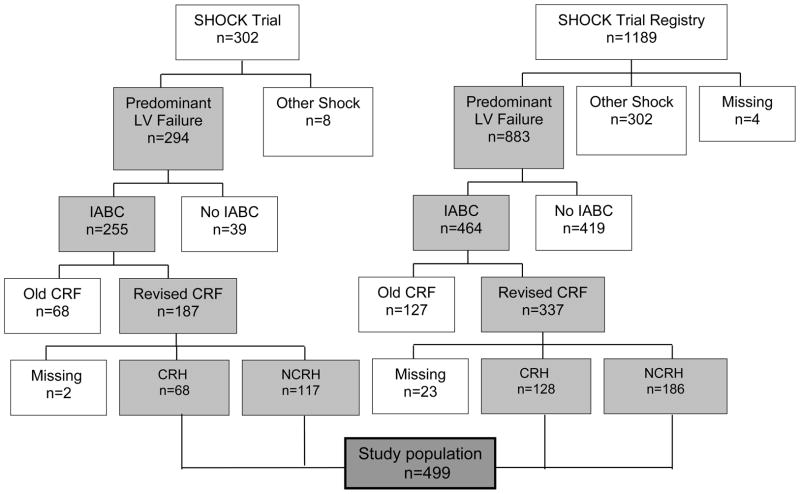
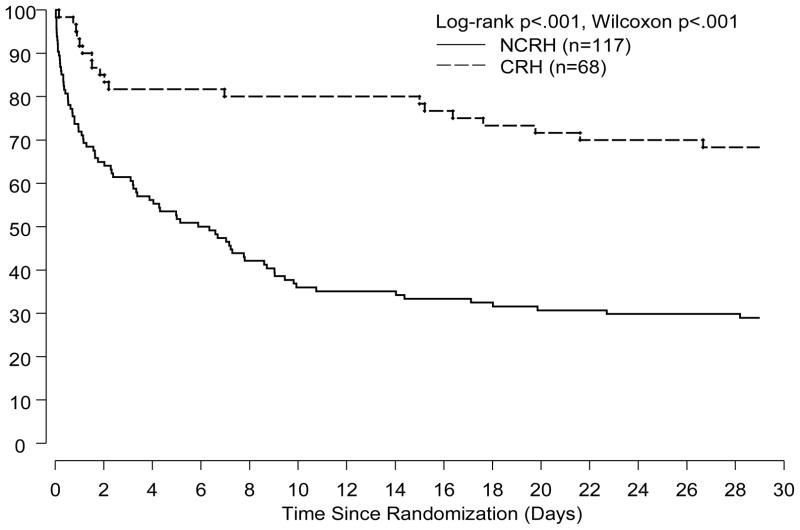
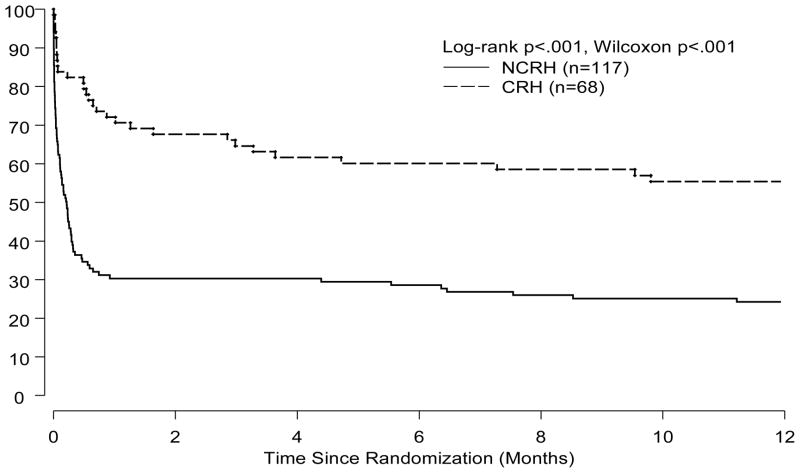
Methods and results: We evaluated 499 patients with record of systemic hypoperfusion status as an early response to IABC from the SHOCK trial (n = 185) and registry (n = 314) to determine the association between rapid complete reversal of systemic hypoperfusion (CRH) after 30 minutes of IABC and in-hospital, 30-day and 1-year mortality. Rapid complete reversal of systemic hypoperfusion was highly associated with lower in-hospital mortality (29% versus 65%, P < .001) in all patients. In the SHOCK trial, among patients assigned to ERV versus IMS, 30-day mortality was 26% versus 29%, respectively, with CRH and 61% versus 81%, respectively, without CRH after commencing IABC. The corresponding 1-year mortality rates were 35% versus 52% for ERV and 69% versus 87% for IMS (interaction P ≥ .25 at both time points). After adjusting for important correlates of outcome (left ventricular ejection fraction, age, and randomization to ERV), a significant association remained between CRH and registry and trial in-hospital mortality (odds ratio 0.23, 95% CI 0.14-0.39, P < .001) and trial 1-year mortality (odds ratio .28, 95% CI 0.12-0.67, P < .001).
Conclusions: In CS patients, CRH after commencing IABC was independently associated with improved in-hospital, 30-day and 1-year survival regardless of early revascularization. In CS patients, CRH with IABC is an important early prognostic feature.
Copyright © 2011 Mosby, Inc. All rights reserved.
Figures
References
-
- Babaev A, Every N, Frederick P, Sichrovsk T, Hochman JS. Trends in revascularization and mortality in patients with cardiogenic shock complicating acute myocardial infarction. Observations from the National Registry of Myocardial Infarction. Circulation. 2002;106:1811.
-
- Hochman JS, Sleeper LA, Webb JG, Sanborn TA, White HD, Talley JD, Buller CE, Jacobs AK, Slater LN, Col J, McKinlay SM, LeJemtel TH for the SHOCK Investigators. N Eng J Med. 1999;341:625–34. - PubMed
-
- Urschel CW, Eder L, Forrester J, Matloff J, Carpenter R, Sonnenblick E. Alterations of mechanical performance of the ventricle by intraaortic ballloon counterpulsation. Am J Cardiol. 1970;25:546–51. - PubMed
-
- Webber KT, Janicki JS. Intraarotic balloon counterpulsation: a review of physiological principles, clinical results and device safety. Ann Thorac Surg. 1974;17:602–36. - PubMed
-
- Anderson RD, Ohman EM, Holmes DR, Col I, Stebbins AL, Bates ER, Stomel RJ, Granger CB, Topol EJ, Califf RM. Use of intraaortic balloon counterpulsation in patients presenting with cardiogenic shock: observations from the GUSTO-1 study. J Am Coll Cardiol. 1997;30:708–15. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
