

Impact of new chemotherapeutic and targeted agents on survival in stage IV non-small cell lung cancer
- PMID: 21835896
- PMCID: PMC3228167
- DOI: 10.1634/theoncologist.2011-0079
Impact of new chemotherapeutic and targeted agents on survival in stage IV non-small cell lung cancer
Abstract
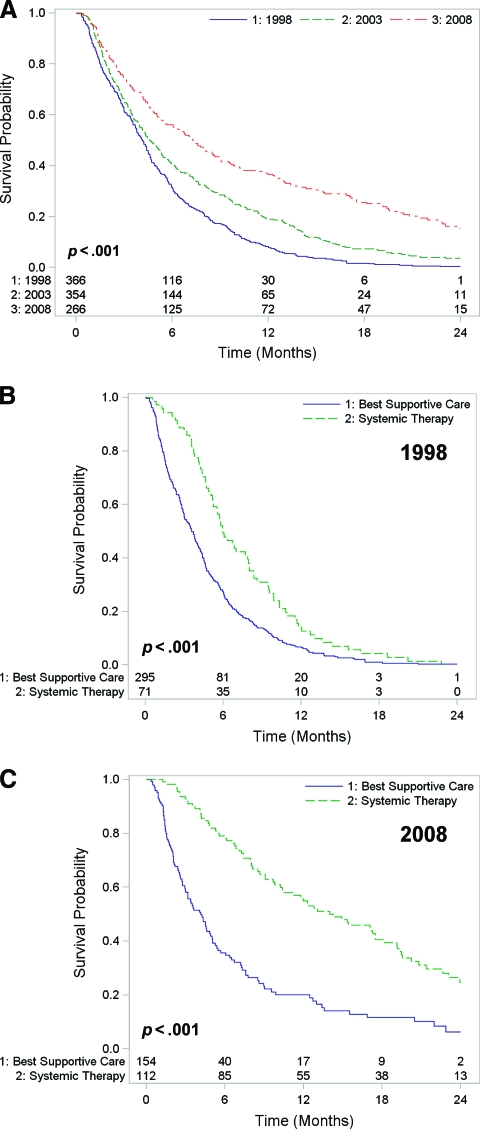
Purpose: Significant advances in the systemic management of metastatic non-small cell lung cancer (NSCLC) have occurred over the past decade, with options now including multiple lines of chemotherapy, epidermal growth factor receptor inhibitors, and antiangiogenic agents. Improvements in overall survival have been demonstrated in randomized controlled trials comparing these newer agents with best supportive care or standard therapy. This study examined uptake of these therapies in general practice and their impact on survival.
Methods: This retrospective cohort study compared demographic, treatment, and survival data among 987 patients diagnosed with stage IV NSCLC at two institutions in 1998, 2003, and 2008. Cohorts were selected based on intervals when doublet chemotherapy, second-line chemotherapy, and targeted agents were incorporated into the standard treatment regimen.
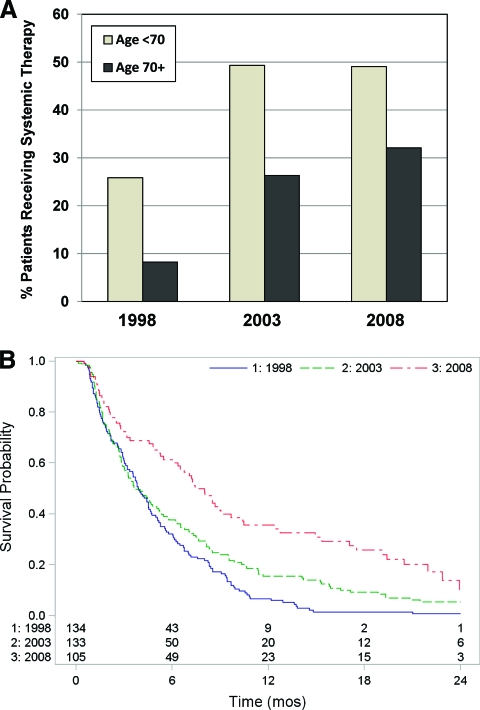
Results: The proportion of patients receiving systemic therapy increased over time (20% in 1998, 42% in 2008). Overall survival improved significantly across cohorts (p < .001), with 2-year survival rates of 0.3% in 1998, 4% in 2003, and 15% in 2008. In a multivariate survival analysis, the 2003 and 2008 cohorts were independently associated with longer survival, as was the use of one or more lines of systemic therapy. Elderly patients (aged ≥70 years) were also more likely to receive systemic therapy over time, with longer overall survival (p < .001).
Conclusion: Over the past decade, there has been an increasing use of systemic therapy in stage IV NSCLC patients, including the elderly. This has been associated with significantly longer overall survival.
Conflict of interest statement
The content of this article has been reviewed by independent peer reviewers to ensure that it is balanced, objective, and free from commercial bias. No financial relationships relevant to the content of this article have been disclosed by the authors or independent peer reviewers.
Figures
References
-
- Altekruse SF, Kosary CL, Krapcho M, et al., editors. SEER Cancer Statistics Review. Bethesda, MD: National Cancer Institute, based on November 2009 SEER data submission, posted to the SEER Web site, 2010; 1975–2007. [accessed February 27, 2011]. Available at http://seer.cancer.gov/csr/1975_2007/
-
- Souquet PJ, Chauvin F, Boissel JP, et al. Polychemotherapy in advanced non small cell lung cancer: A meta-analysis. Lancet. 1993;342:19–21. - PubMed
-
- Schiller JH, Harrington D, Belani CP, et al. Comparison of four chemotherapy regimens for advanced non-small-cell lung cancer. N Engl J Med. 2002;346:92–98. - PubMed
-
- Scagliotti GV, De Marinis F, Rinaldi M, et al. Phase III randomized trial comparing three platinum-based doublets in advanced non-small-cell lung cancer. J Clin Oncol. 2002;20:4285–4291. - PubMed
-
- Shepherd FA, Dancey J, Ramlau R, et al. Prospective randomized trial of docetaxel versus best supportive care in patients with non-small-cell lung cancer previously treated with platinum-based chemotherapy. J Clin Oncol. 2000;18:2095–2103. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
