

Urine sugars for in vivo gut permeability: validation and comparisons in irritable bowel syndrome-diarrhea and controls
- PMID: 21836056
- PMCID: PMC3220318
- DOI: 10.1152/ajpgi.00168.2011
Urine sugars for in vivo gut permeability: validation and comparisons in irritable bowel syndrome-diarrhea and controls
Abstract
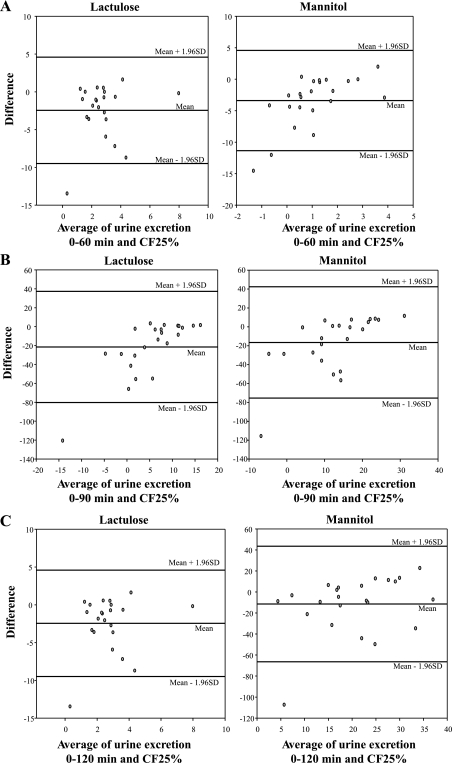
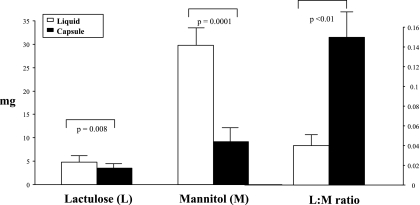
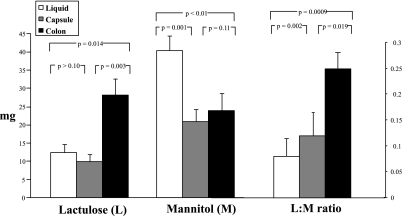
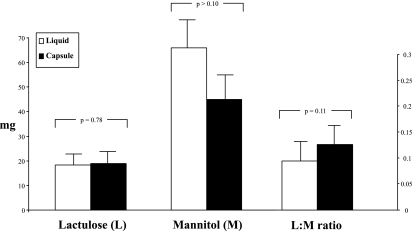
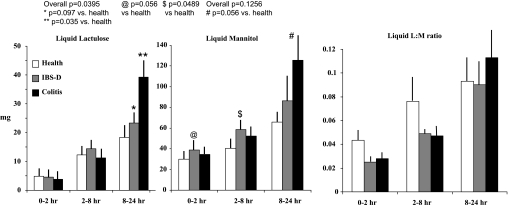
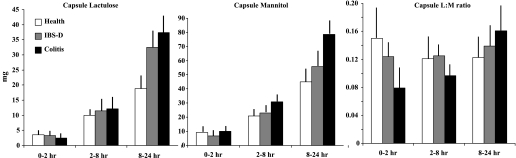
Mucosal barrier dysfunction contributes to gastrointestinal diseases. Our aims were to validate urine sugar excretion as an in vivo test of small bowel (SB) and colonic permeability and to compare permeability in patients with irritable bowel syndrome-diarrhea (IBS-D) to positive and negative controls. Oral lactulose (L) and mannitol (M) were administered with (99m)Tc-oral solution, (111)In-oral delayed-release capsule, or directly into the ascending colon (only in healthy controls). We compared L and M excretion in urine collections at specific times in 12 patients with IBS-D, 12 healthy controls, and 10 patients with inactive or treated ulcerative or microscopic colitis (UC/MC). Sugars were measured by high-performance liquid chromatography-tandem mass spectrometry. Primary endpoints were cumulative 0-2-h, 2-8-h, and 8-24-h urinary sugars. Radioisotopes in the colon at 2 h and 8 h were measured by scintigraphy. Kruskal-Wallis and Wilcoxon tests were used to assess the overall and pairwise associations, respectively, between group and urinary sugars. The liquid in the colon at 2 h and 8 h was as follows: health, 62 ± 9% and 89 ± 3%; IBS-D, 56 ± 11% and 90 ± 3%; and UC/MC, 35 ± 8% and 78 ± 6%, respectively. Liquid formulation was associated with higher M excretion compared with capsule formulation at 0-2 h (health P = 0.049; IBS-D P < 0.001) but not during 8-24 h. UC/MC was associated with increased urine L and M excretion compared with health (but not to IBS-D) at 8-24 h, not at 0-2 h. There were significant differences between IBS-D and health in urine M excretion at 0-2 h and 2-8 h and L excretion at 8-24 h. Urine sugars at 0-2 h and 8-24 h reflect SB and colonic permeability, respectively. IBS-D is associated with increased SB and colonic mucosal permeability.
Figures
References
-
- Anderson AD, Jain PK, Fleming S, Poon P, Mitchell CJ, MacFie J. Evaluation of a triple sugar test of colonic permeability in humans. Acta Physiol Scand 182: 171–177, 2004 - PubMed
-
- Bjarnason I, Hayllar J, MacPherson AJ, Russell AS. Side effects of nonsteroidal anti-inflammatory drugs on the small and large intestine in humans. Gastroenterology 104: 1832–1847, 1993 - PubMed
-
- Bjarnason I, MacPherson A, Hollander D. Intestinal permeability: an overview. Gastroenterology 108: 1566–1581, 1995 - PubMed
-
- Bjarnason I, Peters TJ, Veall N. A persistent defect in intestinal permeability in coeliac disease demonstrated by a 51Cr-labelled EDTA absorption test. Lancet 1: 323–325, 1983 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical