

Termination of respiratory events with and without cortical arousal in obstructive sleep apnea
- PMID: 21836132
- PMCID: PMC3262022
- DOI: 10.1164/rccm.201106-0975OC
Termination of respiratory events with and without cortical arousal in obstructive sleep apnea
Abstract
Rationale: A total of 20-30% of respiratory events in obstructive sleep apnea are terminated without clear arousal. Arousals are thought to predispose to further events by promoting hyperventilation, hypocapnia, and upper-airway dilator muscle hypotonia. Therefore, events terminated without arousal may promote stable breathing.
Objectives: To compare physiologic changes at respiratory event termination with American Sleep Disorders Association (ASDA) Arousal to No Arousal, and determine whether secondary respiratory events are less common and have higher dilator muscle activity after No Arousal compared with ASDA Arousal.
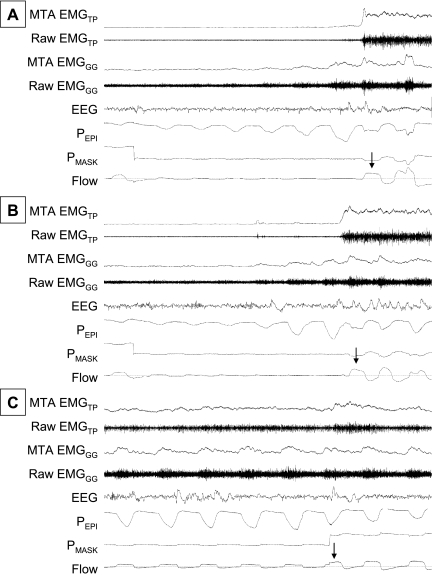
Methods: Patients with obstructive sleep apnea wore sleep staging, genioglossus (EMG(GG)), and tensor palatini (EMG(TP)) electrodes plus a nasal mask and pneumotachograph. During stable sleep, continuous positive airway pressure (CPAP) was lowered for 3-minute periods to induce respiratory events. Physiologic variables were compared between events terminated with (1) ASDA Arousal, (2) No Arousal, or (3) sudden CPAP increase (CPAPinc, control).
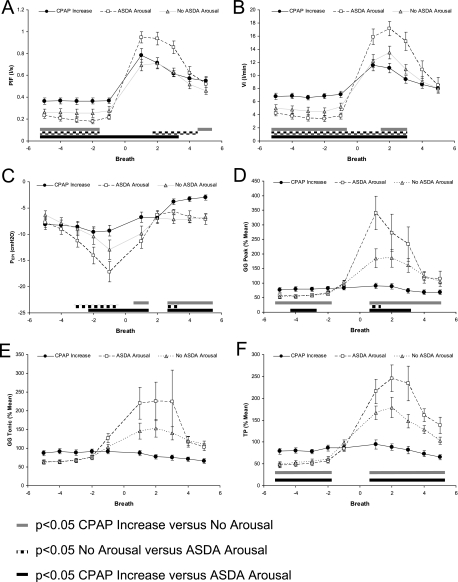
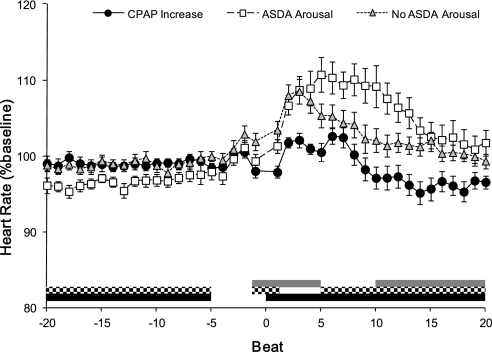
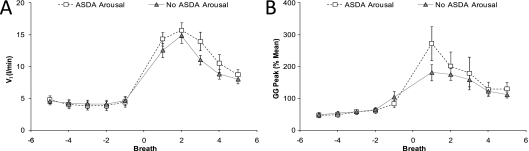
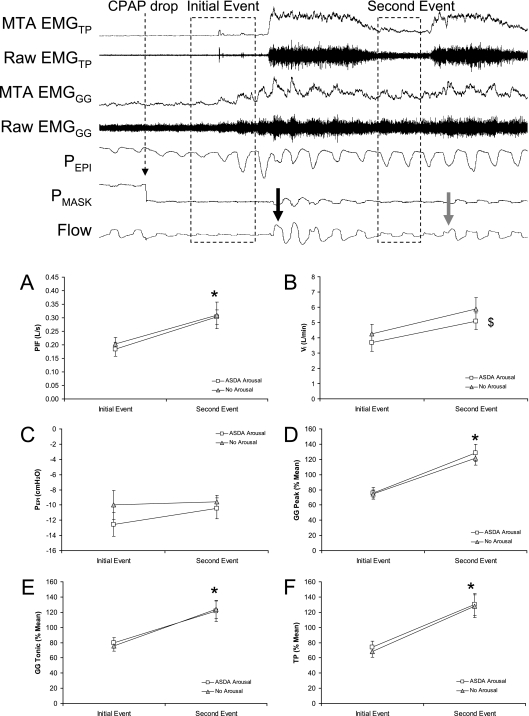
Measurements and main results: Sixteen subjects had adequate data. EMG(GG), EMG(TP), and heart rate increased after ASDA Arousal (340 ± 57%, 215 ± 28%, and 110.7 ± 2.3%) and No Arousal (185 ± 32%, 167 ± 15%, and 108.5 ± 1.6%) but not CPAPinc (90 ± 10%, 94 ± 11%, and 102.1 ± 1%). Ventilation increased more after ASDA Arousal than No Arousal and CPAPinc, but not after accounting for the severity of respiratory event. Fewer No Arousals were followed by secondary events than ASDA Arousals. However, low dilator muscle activity did not occur after ASDA Arousal or No Arousal (EMG(GG) rose from 75 ± 5 to 125 ± 7%) and secondary events were less severe than initial events (ventilation rose 4 ± 0.4 to 5.5 ± 0.51 L/min).
Conclusions: Respiratory events that were terminated with ASDA Arousal were more severely flow-limited, had enhanced hyperventilation after event termination, and were more often followed by secondary events than No arousal. However, secondary events were not associated with low dilator muscle activity and airflow was improved after both No Arousal and ASDA Arousal.
Figures
Comment in
-
Physiologic phenotypes of sleep apnea pathogenesis.Am J Respir Crit Care Med. 2011 Nov 15;184(10):1105-6. doi: 10.1164/rccm.201108-1573ED. Am J Respir Crit Care Med. 2011. PMID: 22086988 Free PMC article. No abstract available.
References
-
- Rees K, Spence DP, Earis JE, Calverley PM. Arousal responses from apneic events during non-rapid-eye-movement sleep. Am J Respir Crit Care Med 1995;152:1016–1021 - PubMed
-
- Dingli K, Fietze I, Assimakopoulos T, Quispe-Bravo S, Witt C, Douglas NJ. Arousability in sleep apnoea/hypopnoea syndrome patients. Eur Respir J 2002;20:733–740 - PubMed
-
- Berry RB, Gleeson K. Respiratory arousal from sleep: mechanisms and significance. Sleep 1997;20:654–675 - PubMed
-
- Younes MK. Role of arousals in the pathogenesis of obstructive sleep apnea. Am J Respir Crit Care Med 2004;169:623–633 - PubMed
-
- Thomas RJ. Arousals in sleep-disordered breathing: patterns and implications. Sleep 2003;26:1042–1047 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
