

Evaluation of admissions to the Major Incident Hospital based on a standardized protocol
- PMID: 21837255
- PMCID: PMC3150834
- DOI: 10.1007/s00068-010-0067-0
Evaluation of admissions to the Major Incident Hospital based on a standardized protocol
Abstract
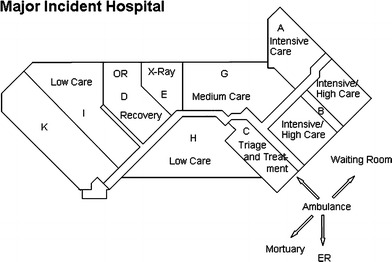
Introduction: The Major Incident Hospital (MIH) is a unique facility strictly reserved to provide immediate large-scale emergency care for victims of disasters and major incidents. We evaluated the implemented organization to identify strengths and weaknesses, and provide knowledge essential for further improvement of preparedness.
Method: According to the Protocol for Reports from Major accidents and Disasters (PRMD) and along with our five scenarios for activation, we analyzed all the data from evaluation reports of all our deployments since the MIH was founded in 1991.
Results: The MIH was able to provide group-wise emergency care to military (29 admissions) as well as civilian victims of major incidents and disasters, both national (260) and international (226). Group-wise treatment was advantageous for quarantine, logistics, registration, emotional support and (pre)arrangements for family, media and security. Strong points are preparedness and availability of a dedicated facility, including ICU, X-ray and OR facilities, irrespective of MRSA status and prearranged cooperation, e.g., with a trauma centre, poison centre and the military. Evaluation, research and training resulted in a barcode registration system and continuous adaptations to improve preparedness. Shortage of resources did not occur; use of the MIH's available resources for national incidents though, could be further optimized.
Conclusions: Recommendations for the future are: improvement of imbedding in regional and national procedures, continued dedicated time and staff for training, research and development, improvement of nuclear/biological/chemical decontamination facilities and preparedness, implementation of standardized scoring systems and expansion of registration systems to the prehospital setting.
Electronic supplementary material: The online version of this article (doi:10.1007/s00068-010-0067-0) contains supplementary material, which is available to authorized users.
Figures








Similar articles
-
Major Incident Hospital: Development of a Permanent Facility for Management of Incident Casualties.Eur J Trauma Emerg Surg. 2009 Jun;35(3):203-11. doi: 10.1007/s00068-009-8230-1. Epub 2009 Mar 16. Eur J Trauma Emerg Surg. 2009. PMID: 26814897
-
Hospital evacuation: Exercise versus reality.Injury. 2016 Sep;47(9):2012-7. doi: 10.1016/j.injury.2016.03.028. Epub 2016 Mar 30. Injury. 2016. PMID: 27084112
-
The future of Cochrane Neonatal.Early Hum Dev. 2020 Nov;150:105191. doi: 10.1016/j.earlhumdev.2020.105191. Epub 2020 Sep 12. Early Hum Dev. 2020. PMID: 33036834
-
Medical management of the traumatic consequences of civil unrest incidents: causation, clinical approaches, needs and advanced planning criteria.Toxicol Rev. 2006;25(3):155-97. doi: 10.2165/00139709-200625030-00003. Toxicol Rev. 2006. PMID: 17192122 Review.
-
Review of Recent Large-Scale Burn Disasters Worldwide in Comparison to Preparedness Guidelines.J Burn Care Res. 2017 Jan/Feb;38(1):36-44. doi: 10.1097/BCR.0000000000000441. J Burn Care Res. 2017. PMID: 27654867 Review.
Cited by
-
Systematic literature review of templates for reporting prehospital major incident medical management.BMJ Open. 2013 Aug 1;3(8):e002658. doi: 10.1136/bmjopen-2013-002658. BMJ Open. 2013. PMID: 23906946 Free PMC article.
-
Burn or trauma scoring: experience of the burn unit of the Queen Astrid Military Hospital during the terror attacks on 22 March 2016.Eur J Trauma Emerg Surg. 2024 Aug;50(4):1611-1619. doi: 10.1007/s00068-024-02486-y. Epub 2024 Mar 20. Eur J Trauma Emerg Surg. 2024. PMID: 38509185
-
Indoor fire in a nursing home: evaluation of the medical response to a mass casualty incident based on a standardized protocol.Eur J Trauma Emerg Surg. 2015 Apr;41(2):167-78. doi: 10.1007/s00068-014-0446-z. Epub 2014 Sep 25. Eur J Trauma Emerg Surg. 2015. PMID: 26038261
References
-
- Bouman JH, Schouwerwou RJ, Van der Eijk KJ, van Leusden AJ, Savelkoul TJ. Computerization of patient tracking and tracing during mass casualty incidents. Eur J Emerg Med Sep. 2000;7(3):211–216. - PubMed
LinkOut - more resources
Full Text Sources
