

Site of deep brain stimulation and jaw velocity in Parkinson disease
- PMID: 21838506
- PMCID: PMC3517909
- DOI: 10.3171/2011.7.JNS102173
Site of deep brain stimulation and jaw velocity in Parkinson disease
Abstract
Object: While deep brain stimulation (DBS) has proven to be an effective treatment for many symptoms of Parkinson disease (PD), a deterioration of axial symptoms frequently occurs, particularly for speech and swallowing. These unfavorable effects of DBS may depend on the site of stimulation. The authors made quantitative measures of jaw velocity to compare the relative effectiveness of DBS in the globus pallidus internus (GPi) or the subthalamic nucleus (STN). This was a randomized, double-blind, and longitudinal study, with matched healthy controls.
Methods: The peak velocities of self-scaled and externally scaled jaw movements were studied in 27 patients with PD before and after 6 months of bilateral DBS in the GPi or the STN. A mixed-effects model was used to identify differences in jaw velocity before DBS surgery (baseline) while off and on levodopa therapy, and after 6 months of DBS (postoperative) during 4 treatment conditions (off- and on-levodopa states with and without DBS).
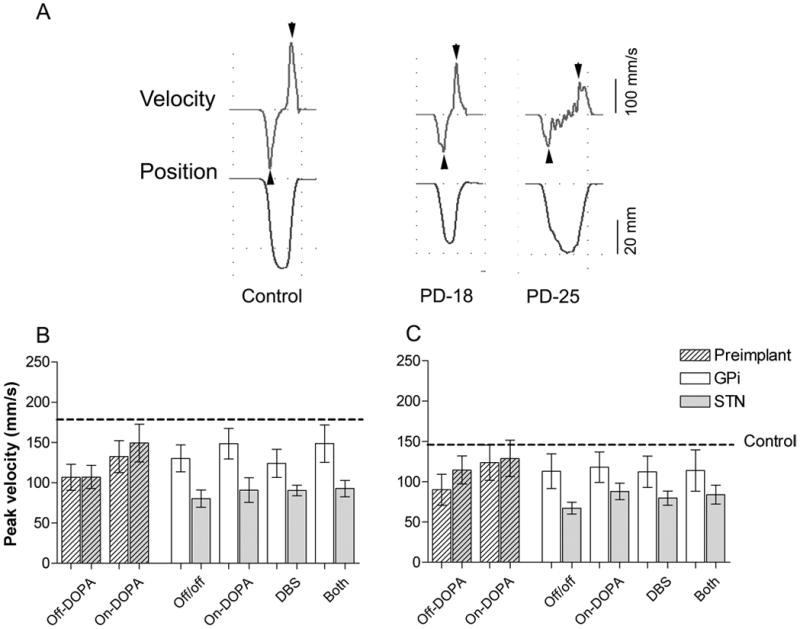
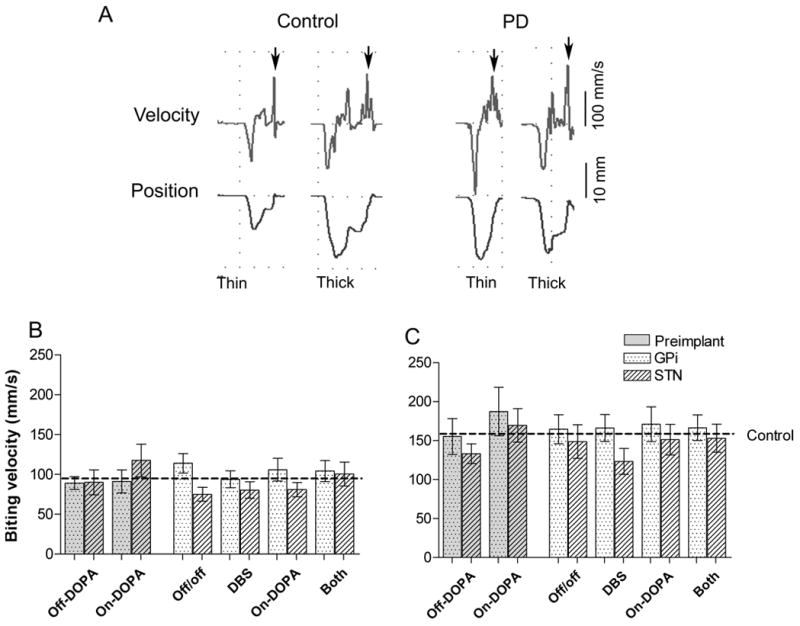
Results: Self-scaled jaw velocity was impaired by the DBS procedure in the STN; velocity was significantly decreased across all postoperative conditions compared with either the off- or on-levodopa baseline conditions. In contrast, the postoperative velocity in the GPi group was generally faster than the baseline off-levodopa state. Turning the DBS off and on had no effect on jaw velocity in either group. Unlike baseline, levodopa therapy postoperatively no longer increased jaw velocity in either group, and this lack of effect was not related to postoperative changes in dose. The externally scaled jaw velocity was little affected by PD, but DBS still slightly affected performance, with the STN group significantly slower than the GPi group for most conditions.
Conclusions: The authors' results suggest that either the electrode implant in STN or the subsequent period of continuous STN stimulation negatively affected voluntary jaw velocity, including the loss of the preoperative levodopa-induced improvement. While the GPi group showed some improvement in voluntary jaw velocity postoperatively, their performance during the combination of DBS and levodopa was not different from their best medical management presurgery. The results have implications for DBS target selection, particularly for those patients with oromotor dysfunctions.
Figures
References
-
- Benabid A, Chabardés S, Seigneuret E. Deep-brain stimulation in Parkinson’s disease: long-term efficacy and safety What happened this year? Cur Opin Neurol. 2005;18:623–630. - PubMed
-
- Ciucci MR, Barkmeier-Kraemer JM, Scherman SJ. Subthalamic nucleus deep brain stimulation improves deglutition in Parkinson’s disease. Mov Disord. 2008;23:676–683. - PubMed
-
- D’Alatri L, Paludetti G, Contarino MF, Galla S, Marchese MR, Bentivoglio AR. Effects of bilateral subthalamic nucleus stimulation and medication on parkinsonian speech impairment. J Voice. 22:365–372. 200. - PubMed
-
- Deuschl G, Herzog J, Kleiner-Fisman G, Kubu C, Lozano AM, Lyons KE, et al. Deep brain stimulation: postoperative issues. Mov Disord Suppl. 2006;14:S219–237. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
