

Withholding and withdrawing life-sustaining therapy in a Moroccan Emergency Department: an observational study
- PMID: 21838861
- PMCID: PMC3199862
- DOI: 10.1186/1471-227X-11-12
Withholding and withdrawing life-sustaining therapy in a Moroccan Emergency Department: an observational study
Abstract
Background: Withdrawing and withholding life-support therapy (WH/WD) are undeniably integrated parts of medical activity. However, Emergency Department (ED) might not be the most appropriate place to give end-of life (EOL) care; the legal aspects and practices of the EOL care in emergency rooms are rarely mentioned in the medical literature and should be studied. The aims of this study were to assess frequency of situations where life-support therapies were withheld or withdrawn and modalities for implement of these decisions.
Method: A survey of patients who died in a Moroccan ED was performed. Confounding variables examined were: Age, gender, chronic underlying diseases, acute medical disorders, APACHE II score, Charlson Comorbidities Index, and Length of stay. If a decision of WH/WD was taken, additional data were collected: Type of decision; reasons supporting the decision, modalities of WH/WD, moment, time from ED admission to decision, and time from processing to withhold or withdrawal life-sustaining treatment to death. Individuals who initiated (single emergency physician, medical staff), and were involved in the decision (nursing staff, patients, and families), and documentation of the decision in the medical record.
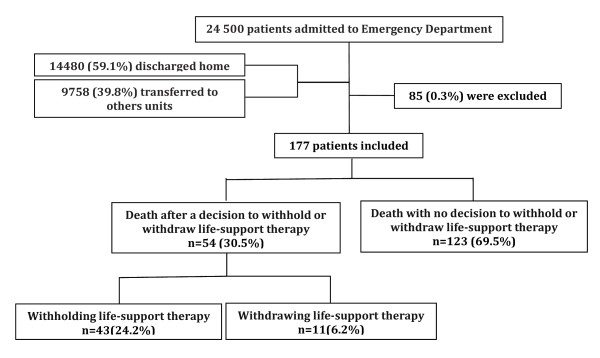
Results: 177 patients who died in ED between November 2009 and March 2010 were included. Withholding and withdrawing life-sustaining treatment was applied to 30.5% of all patients who died. Therapies were withheld in 24.2% and were withdrawn in 6.2%. The most reasons for making these decisions were; absence of improvement following a period of active treatment (61.1%), and expected irreversibility of acute disorder in the first 24 h (42.6%). The most common modalities withheld or withdrawn life-support therapy were mechanical ventilation (17%), vasopressor and inotrops infusion (15.8%). Factors associated with WH/WD decisions were older age (OR = 1.1; 95%IC = 1.01-1.07; P = 0.001), neurological acute medical disorders (OR = 4.1; 95%IC = 1.48-11.68; P = 0.007), malignancy (OR = 7.7; 95%IC = 1.38-8.54; P = 0.002) and cardiovascular (OR = 3.4;95%IC = 2.06-28.5;P = 0.008) chronic underlying diseases.
Conclusion: Life-sustaining treatment were frequently withheld or withdrawn from elderly patients with underlying chronic cardiovascular disease or metastatic cancer or patients with acute neurological medical disorders in a Moroccan ED. Religious beliefs and the lack of guidelines and official Moroccan laws could explain the ethical limitations of the decision-making process recorded in this study.
Figures
Similar articles
-
Withholding and withdrawing life-support therapy in an Emergency Department: prospective survey.Intensive Care Med. 2004 Dec;30(12):2216-21. doi: 10.1007/s00134-004-2475-2. Epub 2004 Oct 29. Intensive Care Med. 2004. PMID: 15517162
-
End of life in ICU--care of the dying or 'pulling the plug'?Ir Med J. 2006 Apr;99(4):112-4. Ir Med J. 2006. PMID: 16972583
-
Withholding and withdrawal of life-sustaining treatment in a Lebanese intensive care unit: a prospective observational study.Intensive Care Med. 2005 Apr;31(4):562-7. doi: 10.1007/s00134-005-2578-4. Epub 2005 Mar 5. Intensive Care Med. 2005. PMID: 15750799
-
Between quality of life and hope. Attitudes and beliefs of Muslim women toward withholding and withdrawing life-sustaining treatments.Med Health Care Philos. 2018 Sep;21(3):347-361. doi: 10.1007/s11019-017-9808-8. Med Health Care Philos. 2018. PMID: 29043540 Review.
-
Withholding and withdrawal of life support: ethical, legal, and clinical aspects.New Horiz. 1997 Feb;5(1):30-7. New Horiz. 1997. PMID: 9017676 Review.
Cited by
-
Critical care research in Morocco and Tunisia.Intensive Care Med. 2018 Apr;44(4):502-505. doi: 10.1007/s00134-018-5099-7. Epub 2018 Mar 8. Intensive Care Med. 2018. PMID: 29520659 No abstract available.
-
Pragmatic methods to avoid intensive care unit admission when it does not align with patient and family goals.Lancet Respir Med. 2019 Jul;7(7):613-625. doi: 10.1016/S2213-2600(19)30170-5. Epub 2019 May 20. Lancet Respir Med. 2019. PMID: 31122895 Free PMC article. Review.
-
Limitation of therapeutic effort experienced by intensive care nurses.Nurs Ethics. 2018 Nov;25(7):867-879. doi: 10.1177/0969733016679471. Epub 2016 Dec 28. Nurs Ethics. 2018. PMID: 28027690 Free PMC article.
-
Ethical aspects of limiting end-of-Life treatment of adult patients at the primary healthcare level in family and emergency medicine: a systematic review.BMC Palliat Care. 2025 Jul 1;24(1):169. doi: 10.1186/s12904-025-01807-1. BMC Palliat Care. 2025. PMID: 40597127 Free PMC article.
-
The end-of-life care in the emergency department setting with respect to the Middle East countries and comparison with the Western countries.Turk J Emerg Med. 2022 Jan 20;22(1):1-7. doi: 10.4103/2452-2473.336105. eCollection 2022 Jan-Mar. Turk J Emerg Med. 2022. PMID: 35284692 Free PMC article. Review.
References
-
- Pochard F, Azoulay E, Chevret S, Lemaire F, Hubert P, Canoui P, Grassin M, Zittoun R, Le Gall JR, Dhainaut JF, Schlemmer B. for the French FAMIREA group. Symptoms of anxiety and depression in family members of intensive care unit patients: ethical hypothesis regarding decision-making capacity. Crit Care Med. 2001;29:1893–7. doi: 10.1097/00003246-200110000-00007. - DOI - PubMed
-
- Bone RC, Rackow EC, Weg JG. Ethical and moral guidelines for the initiation, continuation, and withdrawal of intensive care. Chest. 1990;97:949–57. - PubMed
-
- Grudzen CR, Stone SC, Mohanty SA, Asch SM, Lorenz KA, Torres JM, Morrison M, Ortiz JM, Timmermans S. 'I Want to be taking my own last breath'': patients' reflections on illness when presenting to the Emergency Department at the end of life. J Palliat Med. 2011;14:293–6. doi: 10.1089/jpm.2010.0306. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
