

Impaired mitochondrial biogenesis precedes heart failure in right ventricular hypertrophy in congenital heart disease
- PMID: 21840936
- PMCID: PMC3218261
- DOI: 10.1161/CIRCHEARTFAILURE.111.961474
Impaired mitochondrial biogenesis precedes heart failure in right ventricular hypertrophy in congenital heart disease
Abstract
Background: The outcome of the surgical repair in congenital heart disease correlates with the degree of myocardial damage. In this study, we determined whether mitochondrial DNA depletion is a sensitive marker of right ventricular (RV) damage and whether impaired mitochondrial DNA (mtDNA) replication contributes to the transition from compensated hypertrophy to failure.
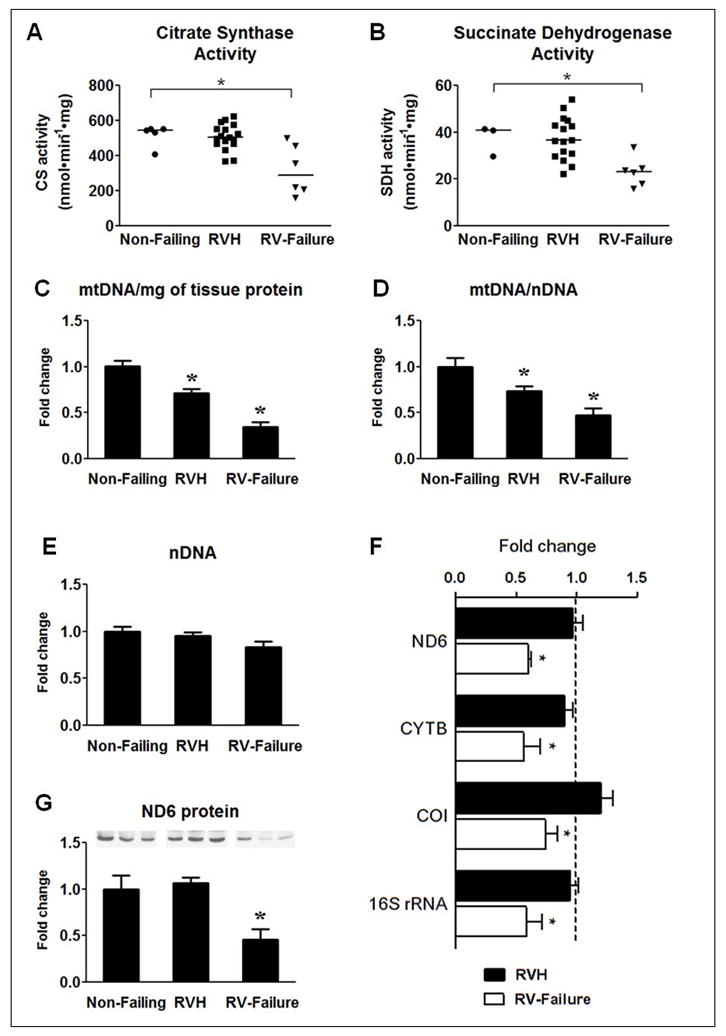
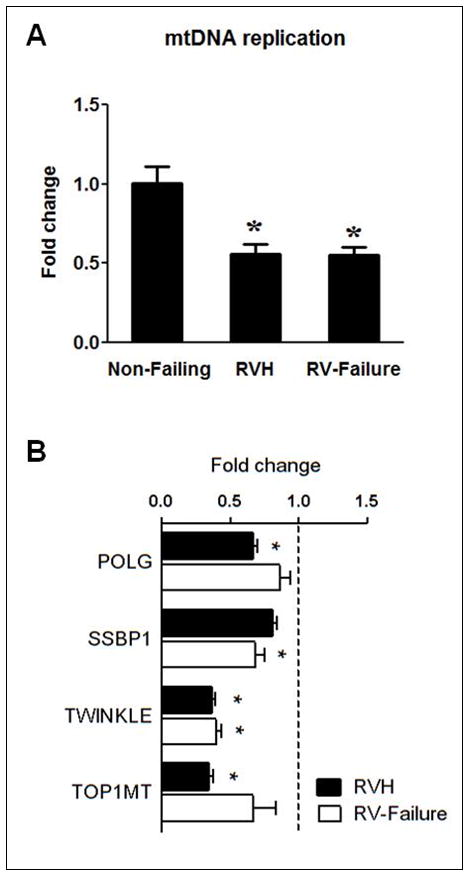
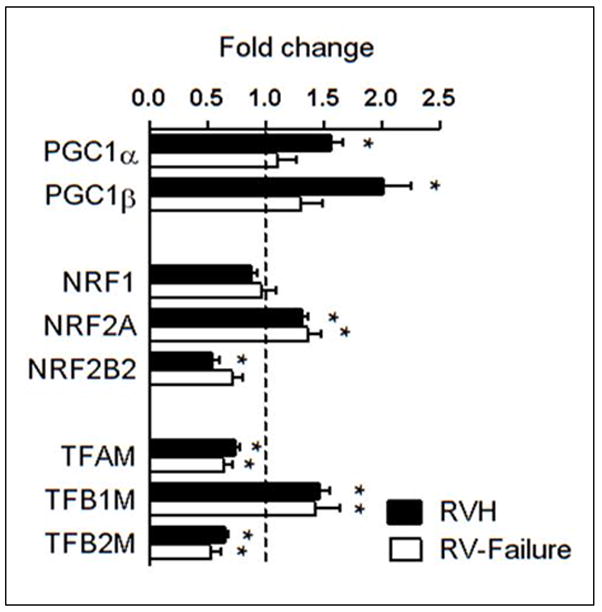
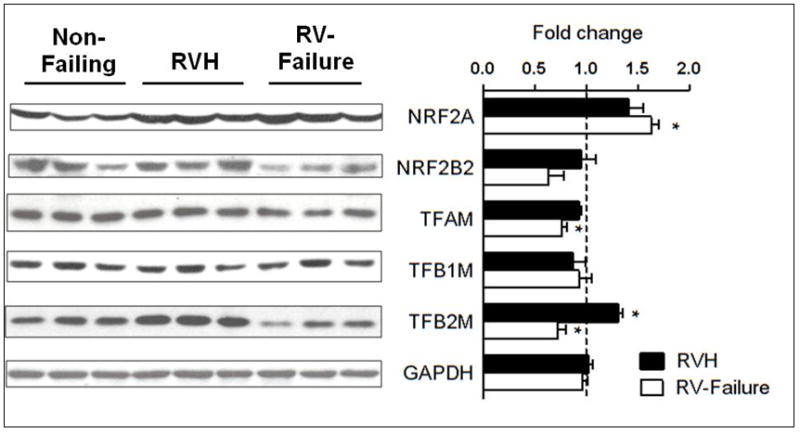
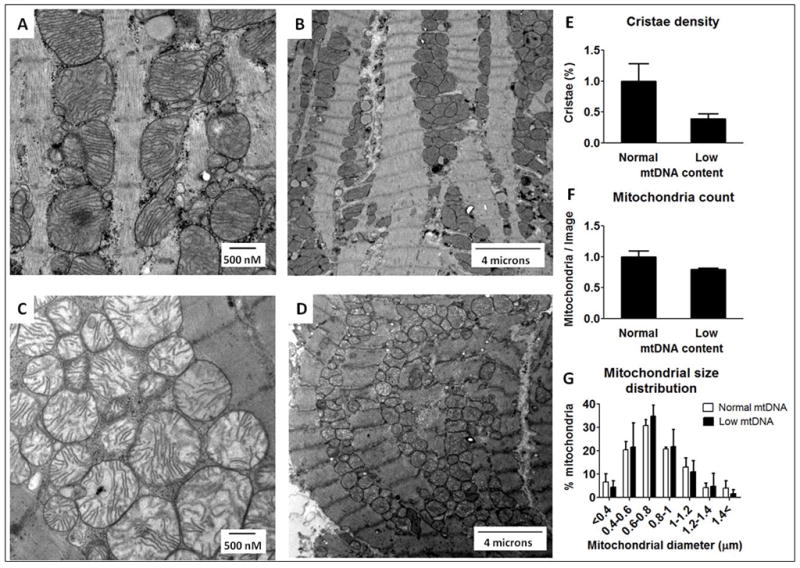
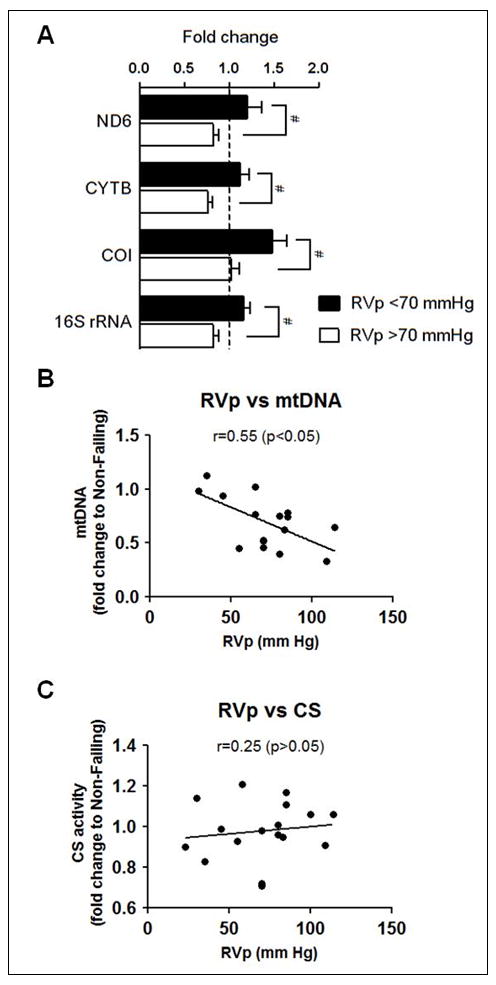
Methods and results: RV samples obtained from 31 patients undergoing cardiac surgery were compared with 5 RV samples from nonfailing hearts (control). Patients were divided into compensated hypertrophy and failure groups, based on preoperative echocardiography, catheterization, and/or MRI data. Mitochondrial enzyme activities (citrate synthase and succinate dehydrogenase) were maintained during hypertrophy and decreased by ≈40% (P<0.05 versus control) at the stage of failure. In contrast, mtDNA content was progressively decreased in the hypertrophied RV through failure (by 28±8% and 67±11%, respectively, P<0.05 for both), whereas mtDNA-encoded gene expression was sustained by increased transcriptional activity during compensated hypertrophy but not in failure. Mitochondrial DNA depletion was attributed to reduced mtDNA replication in both hypertrophied and failing RV, and it was independent of PGC-1 downregulation but was accompanied by reduced expression of proteins constituting the mtDNA replication fork. Decreased mtDNA content in compensated hypertrophy was also associated with pathological changes of mitochondria ultrastructure.
Conclusions: Impaired mtDNA replication causes early and progressive depletion of mtDNA in the RV of the patients with congenital heart disease during the transition from hypertrophy to failure. Decreased mtDNA content probably is a sensitive marker of mitochondrial injury in this patient population.
Figures
Comment in
-
Letter by Pohjoismaki regarding article, "Impaired mitochondrial biogenesis precedes heart failure in right ventricular hypertrophy in congenital heart disease".Circ Heart Fail. 2012 Jan;5(1):e15; author reply e16. doi: 10.1161/CIRCHEARTFAILURE.111.964502. Circ Heart Fail. 2012. PMID: 22253409 No abstract available.
References
-
- Murphy JG, Gersh BJ, Mair DD, Fuster V, McGoon MD, Ilstrup DM, McGoon DC, Kirklin JW, Danielson GK. Long-term outcome in patients undergoing surgical repair of tetralogy of Fallot. N Engl J Med. 1993;329:593–599. - PubMed
-
- Therrien J, Siu SC, McLaughlin PR, Liu PP, Williams WG, Webb GD. Pulmonary valve replacement in adults late after repair of tetralogy of fallot: are we operating too late? J Am Coll Cardiol. 2000;36:1670–1675. - PubMed
-
- Bouzas B, Kilner PJ, Gatzoulis MA. Pulmonary regurgitation: not a benign lesion. Eur Heart J. 2005;26:433–439. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
