

Metabolic abnormalities, cardiovascular disease risk factors, and GFR decline in children with chronic kidney disease
- PMID: 21841064
- PMCID: PMC3358991
- DOI: 10.2215/CJN.07100810
Metabolic abnormalities, cardiovascular disease risk factors, and GFR decline in children with chronic kidney disease
Erratum in
- Clin J Am Soc Nephrol. 2014 May;9(5):997-8
Abstract
Background and objectives: Metabolic abnormalities and cardiovascular disease (CVD) risk factors have rarely been systematically assessed in children with chronic kidney disease (CKD). We examined the prevalence of various CKD sequelae across the GFR spectrum.
Design, setting, participants, & measurements: Data were used from 586 children participating in the Chronic Kidney Disease in Children (CKiD) study (United States and Canada) with GFR measured by iohexol plasma disappearance. Laboratory values and CVD risk factors were compared across GFR categories and with an age-, gender-, and race-matched community sample.
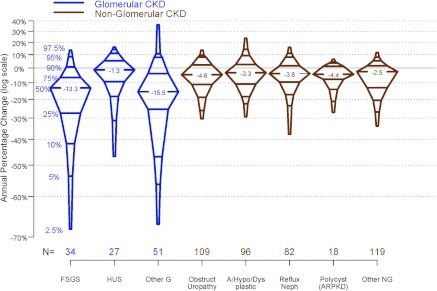
Results: CKiD participants were 62% male, 66% Caucasian, 23% African American, and 15% Hispanic with a median age of 11 years and a median GFR of 44 ml/min per 1.73 m(2). Compared with those with a GFR ≥ 50 ml/min per 1.73 m(2), having a GFR < 30 ml/min per 1.73 m(2) was associated with a three-fold higher risk of acidosis and growth failure and a four- to five-fold higher risk of anemia and elevated potassium and phosphate. Median GFR change was -4.3 ml/min per 1.73 m(2) and -1.5 ml/min per 1.73 m(2) per year in children with glomerular and nonglomerular diagnoses, respectively. Despite medication and access to nephrology care, uncontrolled systolic hypertension was present in 14%, and 16% had left ventricular hypertrophy. Children with CKD frequently were also shorter and had lower birth weight, on average, compared with norms.
Conclusions: Growth failure, metabolic abnormalities, and CVD risk factors are present at GFR >50 ml/min per 1.73 m(2) in children with CKD and, despite therapy, increase in prevalence two- to four-fold with decreasing GFR.
Figures
References
-
- Collins AJ, Foley RN, Herzog C, Chavers B, Gilbertson D, Ishani A, Kasiske B, Liu J, Mau LW, McBean M, Murray A, St Peter W, Guo H, Gustafson S, Li Q, Li S, Peng Y, Qiu Y, Roberts T, Skeans M, Snyder J, Solid C, Wang C, Weinhandl E, Zaun D, Arko C, Chen SC, Dalleska F, Daniels F, Dunning S, Ebben J, Frazier E, Hanzlik C, Johnson R, Sheets D, Wang X, Forrest B, Constantini E, Everson S, Eggers P, Agodoa L: U.S. Renal Data System 2010 Annual Data Report. Am J Kidney Dis 57: A8, 2011 - PubMed
-
- Schwartz GJ, Haycock GB, Edelmann CM, Jr, Spitzer A: A simple estimate of glomerular filtration rate in children derived from body length and plasma creatinine. Pediatrics, 58: 259–263, 1976 - PubMed
-
- The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics 114: 555–576, 2004 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
