

Assessing the impact of screening colonoscopy on mortality in the medicare population
- PMID: 21842323
- PMCID: PMC3235614
- DOI: 10.1007/s11606-011-1816-4
Assessing the impact of screening colonoscopy on mortality in the medicare population
Abstract
Background: Some have recommended against routine screening for colorectal cancer (CRC) among patients ≥75 years of age, while others have suggested that screening colonoscopy (SC) is less beneficial for women than men. We estimated the expected benefits (decreased mortality from CRC) and harms (SC-related mortality) of SC based on sex, age, and comorbidity.
Objective: To stratify older patients according to expected benefits and harms of SC based on sex, age, and comorbidity.
Design: Retrospective study using Medicare claims data.
Participants: Medicare beneficiaries 67-94 years old with and without CRC.
Main measures: Life expectancy, CRC- and colonoscopy-attributable mortality rates across strata of sex, age, and comorbidity, pay-off time (i.e. the minimum time until benefits from SC exceeded harms), and life-years saved for every 100,000 SC.
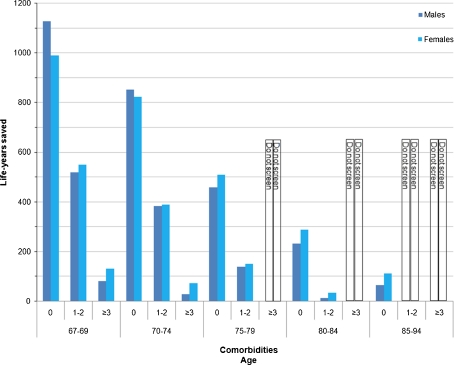
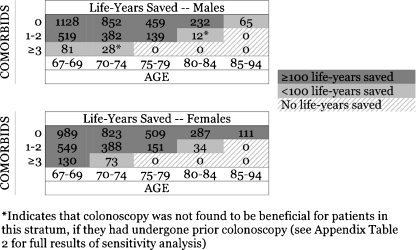
Key results: Increasing age and comorbidity were associated with lower CRC-attributable mortality. Due to shorter life expectancy and CRC-attributable mortality, the benefits associated with SC were substantially lower among patients with greater comorbidity. Among men aged 75-79 years with no comorbidity, the number of life-years saved was 459 per 100,000 SC, while men aged 67-69 with ≥3 comorbidities had 81 life-years saved per 100,000 SC. There was no evidence that SC was less effective in women. Among men and women 75-79 with no comorbidity, number of life-years saved was 459 and 509 per 100,000 SC, respectively; among patients with ≥3 comorbidities, there was no benefit for either men or women.
Conclusions: Although the effectiveness of SC was equivalent for men and women, there was substantial variation in SC effectiveness within age groups, arguing against screening recommendations based solely on age.
Figures
Comment in
-
Individualized screening for colorectal cancer: one size does not fit all.Gastroenterology. 2012 Mar;142(3):672-3. doi: 10.1053/j.gastro.2012.01.021. Epub 2012 Jan 24. Gastroenterology. 2012. PMID: 22281275 No abstract available.
References
-
- Force USPST Screening for colorectal cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2008;149(9):627–637. - PubMed
-
- (CDC) CfDCaP. Behavioral Risk Factor Surveillance System Survey Data. Vol. 2009. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention; 2009.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
