

Cardiovascular events in early RA are a result of inflammatory burden and traditional risk factors: a five year prospective study
- PMID: 21843325
- PMCID: PMC3239373
- DOI: 10.1186/ar3442
Cardiovascular events in early RA are a result of inflammatory burden and traditional risk factors: a five year prospective study
Abstract
Introduction: Co-morbidity and mortality due to cardiovascular disease (CVD) are increased in patients with rheumatoid arthritis (RA). Most published studies in this field are retrospective or cross sectional. We investigated the presence of traditional and disease related risk factors for CVD at the onset of RA and during the first five years following diagnosis. We also evaluated their potential for predicting a new cardiovascular event (CVE) during the five-year follow-up period and the modulatory effect of pharmacological treatment.
Methods: All patients from the four northern-most counties of Sweden with early RA are, since December 1995, consecutively recruited at diagnosis (T0) into a large survey on the progress of the disease. Information regarding cardiovascular co-morbidity and related predictors was collected from clinical records and supplemented with questionnaires. By April 2008, 700 patients had been included of whom 442 patients had reached the five-year follow-up (T5).
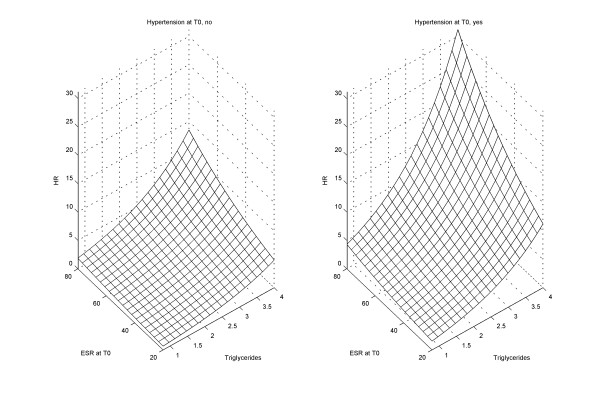
Results: Among the 442 patients who reached T5 during the follow-up period, treatment for hypertension increased from 24.5 to 37.4% (P < 0.001)), diagnosis of diabetes mellitus (DM) from 7.1 to 9.5% (P < 0.01) whilst smoking decreased from 29.8 to 22.4% (P < 0.001) and the BMI from 26.3 to 25.8 (P < 0.05), respectively. By T5, 48 patients had suffered a new CVE of which 12 were fatal. A total of 23 patients died during the follow-up period. Age at disease onset, male sex, a previous CVE, DM, treatment for hypertension, triglyceride level, cumulative disease activity (area under the curve (AUC) disease activity score (DAS28)), extra-articular disease, corticosteroid use, shorter duration of treatment with disease modifying anti-rheumatic drugs (DMARDs) and use of COX-2 inhibitors increased the hazard rate for a new CVE. A raised erythrocyte sedimentation rate (ESR) at inclusion and AUC DAS28 at six months increased the hazard rate of CVE independently whilst DMARD treatment was protective in multiple Cox extended models adjusted for sex and CV risk factors. The risk of a CVE due to inflammation was potentiated by traditional CV risk factors.
Conclusions: The occurrence of new CV events in very early RA was explained by traditional CV risk factors and was potentiated by high disease activity. Treatment with DMARDs decreased the risk. The results may have implications for cardio-protective strategies in RA.
Figures
References
-
- Myllykangas-Luosujärvi R, Aho K, Kautiainen H, Isomäki H. Cardiovascular mortality in women with rheumatoid arthritis. J Rheumatol. 1995;22:1065–1067. - PubMed
-
- Wållberg-Jonsson S, Öhman ML, Rantapää-Dahlqvist S. Cardiovascular morbidity and mortality in patients with seropositive rheumatoid arthritis in Northern Sweden. J Rheumatol. 1997;24:445–451. - PubMed
-
- Björnådal L, Baecklund E, Yin L, Granath F, Klareskog L, Ekbom A. Decreasing mortality in patients with rheumatoid arthritis: results from a large population based cohort in Sweden, 1964-95. J Rheumatol. 2002;29:906–912. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
