

Molecular serum portraits in patients with primary breast cancer predict the development of distant metastases
- PMID: 21844363
- PMCID: PMC3161545
- DOI: 10.1073/pnas.1103125108
Molecular serum portraits in patients with primary breast cancer predict the development of distant metastases
Abstract
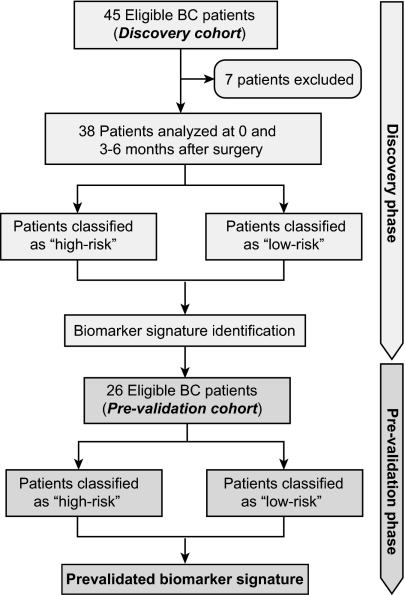
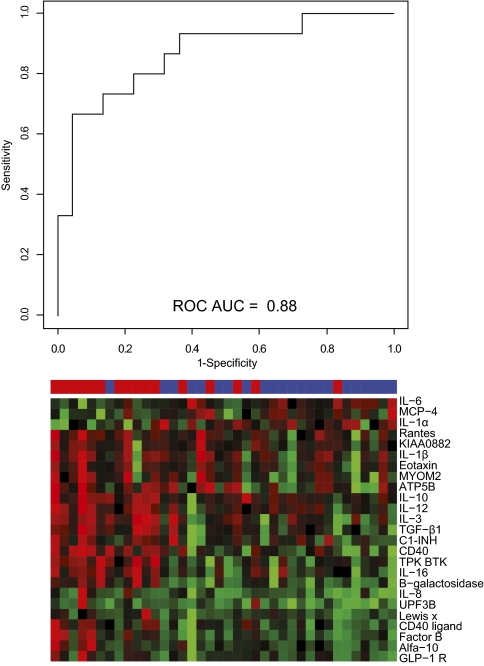
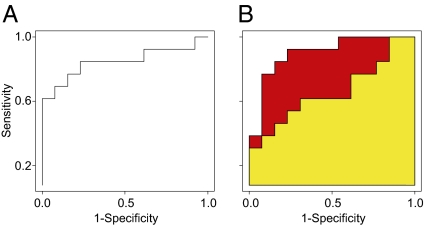
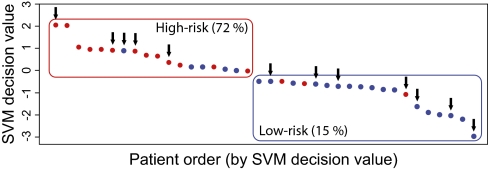
The risk of distant recurrence in breast cancer patients is difficult to assess with current clinical and histopathological parameters, and no validated serum biomarkers currently exist. Using a recently developed recombinant antibody microarray platform containing 135 antibodies against 65 mainly immunoregulatory proteins, we screened 240 sera from 64 patients with primary breast cancer. This unique longitudinal sample material was collected from each patient between 0 and 36 mo after the primary operation. The velocity for each serum protein was determined by comparing the samples collected at the primary operation and then 3-6 mo later. A 21-protein signature was identified, using leave-one-out cross-validation together with a backward elimination strategy in a training cohort. This signature was tested and evaluated subsequently in an independent test cohort (prevalidation). The risk of developing distant recurrence after primary operation could be assessed for each patient, using her molecular portraits. The results from this prevalidation study showed that patients could be classified into high- versus low-risk groups for developing metastatic breast cancer with a receiver operating characteristic area under the curve of 0.85. This risk assessment was not dependent on the type of adjuvant therapy received by the patients. Even more importantly, we demonstrated that this protein signature provided an added value compared with conventional clinical parameters. Consequently, we present here a candidate serum biomarker signature able to classify patients with primary breast cancer according to their risk of developing distant recurrence, with an accuracy outperforming current procedures.
Conflict of interest statement
Conflict of interest statement: Patent application on the biomarker signature (C.A.K.B. and C.W.).
Figures
References
-
- Jemal A, et al. Cancer statistics, 2009. CA Cancer J Clin. 2009;59:225–249. - PubMed
-
- La Vecchia C, et al. Cancer mortality in Europe, 2000-2004, and an overview of trends since 1975. Ann Oncol. 2010;21:1323–1360. - PubMed
-
- Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: An overview of the randomised trials. Lancet. 2005;365:1687–1717. - PubMed
-
- Dowsett M, et al. Meta-analysis of breast cancer outcomes in adjuvant trials of aromatase inhibitors versus tamoxifen. J Clin Oncol. 2010;28:509–518. - PubMed
-
- Gonzalez-Angulo AM, Morales-Vasquez F, Hortobagyi GN. Overview of resistance to systemic therapy in patients with breast cancer. Adv Exp Med Biol. 2007;608:1–22. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
