

Primary pulmonary malignancy: treatment by total pneumonectomy; analysis of 79 collected cases and presentation of 7 personal cases
Affiliations
- PMID: 21845128
- PMCID: PMC3145446
Item in Clipboard
Primary pulmonary malignancy: treatment by total pneumonectomy; analysis of 79 collected cases and presentation of 7 personal cases
Ochsner J.
1999 Jul.
No abstract available
Figures

Lining cells of tracheal mucosa of a fetus 12 centimeters long. Beneath the cylindrical cells covering the surface there are several rows of nuclei of “reserve cells.” Modified after D'Aunoy, Pearson, and Halpert (13, 26).

The “reserve cell” is the parent cell of the ciliated cylindrical and goblet cells, and also possesses the qualities of its ancestor cell in that it may differentiate into any kind of epithelial cell that a primitive entodermal cell is capable of producing. Hence, the carcinomas of the lung may be: (1) “reserve-cell” carcinoma, (2) cylindrical-cell carcinoma, and (3) squamous-cell carcinoma. Modified after D'Aunoy, Pearson, and Halpert (13, 26).

“Reserve-cell” carcinomas grow in solid masses composed of round, elongated (oat cells) or polygonal cells forming no particular structure. Usually there is a palisade arrangement of the peripheral cells. Modified after D'Aunoy, Pearson, and Halpert (13, 26).

Cylindrical cell carcinomas are composed of cuboidal or columnar cells forming acinar, tubular, or papillary structures. The parent cells are the “reserve cells” which form haphazard imitations of the normal epithelial cell structure which composes the air passages. Modified after the method of D'Aunoy, Pearson, and Halpert (13, 26).

Squamous cell carcinomas grow in nests of cells in a concentric arrangement forming epithelial pearls with central keratinization. The entodermal cell of the air passages has the quality of producing stratified squamous epithelium. The parent cell of this carcinoma is a “reserve cell” of earlier ancestry than the ordinary. Modified after D'Aunoy, Pearson, and Halpert (13, 26).

Anteroposterior roentgenogram of chest of patient with carconoma involving right lower lobe bronchus as characterized by slightly rounded but irregular shadow in lower right lung field adjacent to hilum. The mediastinum is displaced slightly toward the affected side (Case 3).

Anteroposterior roentgenogram of chest of patient with carcinoma of right upper lobe bronchus which had extended peripherally to involve practically the entire lobe as confirmed by subsequent examination. The area of increased density; occupying nearly the whole upper lobe of the right lung, is produced by the peripheral extension of the tumor and not by atelectasis which would cause displacement of the mediastinum toward the affected side (Case 2).

Drawing illustrating site of skin incision over third rib from chondrosternal junction to anterior axillary line in anterior approach for pneumonectomy.

Drawing illustrating anterior approach for pneumonectomy. The third rib is resected subperiosteally from chondrosternal junction to anterior axillary line. Incision of the pleura is made in the bed of the third rib. Inset shows exposure and immediate ligation of internal mammary vessels.

Drawing showing position of patient in posterior approach for pneumonectomy.

Drawing illustrating skin incision in posterior approach for penumonectomy as devised by Crafoord. The incision begins over the fourth rib about 7 to 8 centimeters from the posterior midline, is extended downward beneath the angle of the scapula, and then up toward the midaxillary line to the level of the fifth rib which is followed anteriorly to the costal cartilage.

Drawing showing method of elevating angle of scapula so as to expose the fifth rib along its entire length. The fifth rib is subperiosteally resected throughout its entire length and the pleura is opened by incising in the furrow left by the rib.

Drawing showing relation of hilar structures and steps of operation in posterior approach for pneumonectomy. The hilar structures are exposed by incising mediastinal pleura posteriorly and superiorly. The azygos vein is first exposed, doubly transfixed and ligated, and then divided between these ligatures. This permits easy access to the bronchus which is doubly clamped by means of crushing forceps and divided between the clamps. Following division of bronchus, which normally holds the hilar structures quite rigidly, dissection of the other hilar structures, the pulmonary artery and veins, is greatly facilitated.

Drawing showing incision of mediastinal pleura in anterior approach for pneumonectomy. Mobilization of flaps of mediastinal pleura is greatly facilitated by use of long ball-tipped, slightly curved scissors.

Drawing showing individual isolation of pulmonary artery, pulmonary vein, and bronchus in anterior approach for pneumonectomy.

Diagrammatic illustration of futility of mass ligation and necessity of high section of bronchus as exemplified in authors' first case. Although individual ligation of hilar structures was done, the bronchus was divided insufficiently high to include the tumor. The pathologist, who was present at the operation, observed absence of tumor before mediastinal wound was closed, permitting further dissection of bronchus up to carina and high removal of bronchus to include tumor.

Diagrammatic illustration of technique which is employed in individual isolation of hilar structures. Division of the pulmonary artery and of the pulmonary veins is performed between double ligation and transfixion sutures.

Drawing showing pleuralization of mediastinum following complete extirpation of all mediastinal lymph nodes. The edges of the divided mediastinal pleura are approximated covering the stump of the ligated vessels and bronchus with pleura.

Graphic representation of total mortality in 86 collected cases of pneumonectomy for neoplastic disease, including 7 performed by the authors.

Graphic representation of age incidence according to decades in 50 collected cases of pneumonectomy including authors'

Graphic representation of sex incidence in 51 collected cases of pneumonectomy including authors'.

Graphic representation of localization, according to side involved, of pulmonary neoplasms in 53 collected cases of pneumonectomy including authors'.

Graphic representation of mortality in 48 collected cases of pneumonectomy including authors', according to treatment of hilar structures.

Graphic representation of cause of death in 38 collected cases of pneumonectomy including authors'.
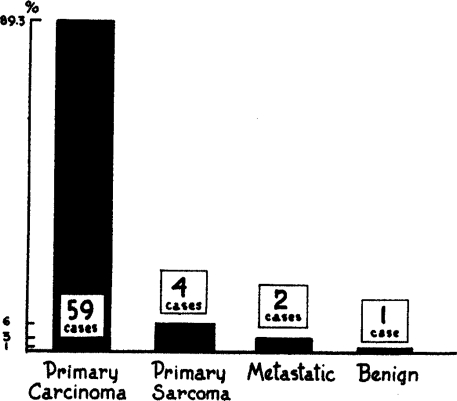
Graphic representation of type of neoplasm in 66 collected cases of pneumonectomy including authors'.

Graphic representation of mortality in 53 collected cases of pneumonectomy including authors', according to side of operation.
References
-
- Alexander J. Personal communication to Haight. Surg., Gynec. & Obst., 1934;58
-
- Arce M. J. Pneumectomie totale (Le tampon-drainage en chirurgie endothoracique). Mém. Acad. de Chir., 1936;62
-
- Idem. Tratamiento quirurgico de los quiste y tumores del pulmón (metodos y procedemuntos generates) Soc. Internat de Chir., 11th Congress, Sept. 1938.
LinkOut - more resources
Full Text Sources