

Variation in reoperation after colorectal surgery in England as an indicator of surgical performance: retrospective analysis of Hospital Episode Statistics
- PMID: 21846714
- PMCID: PMC3156827
- DOI: 10.1136/bmj.d4836
Variation in reoperation after colorectal surgery in England as an indicator of surgical performance: retrospective analysis of Hospital Episode Statistics
Abstract
Objective: To describe national reoperation rates after elective and emergency colorectal resection and to assess the feasibility of using reoperation as a quality indicator derived from routinely collected data in England.
Design: Retrospective observational study of Hospital Episode Statistics (HES) data.
Setting: HES dataset, an administrative dataset covering the entire English National Health Service.
Participants: All patients undergoing a primary colorectal resection in England between 2000 and 2008.
Main outcome measures: Reoperation after colorectal resection, defined as any reoperation for an intra-abdominal procedure or wound complication within 28 days of surgery on the index or subsequent admission to hospital.
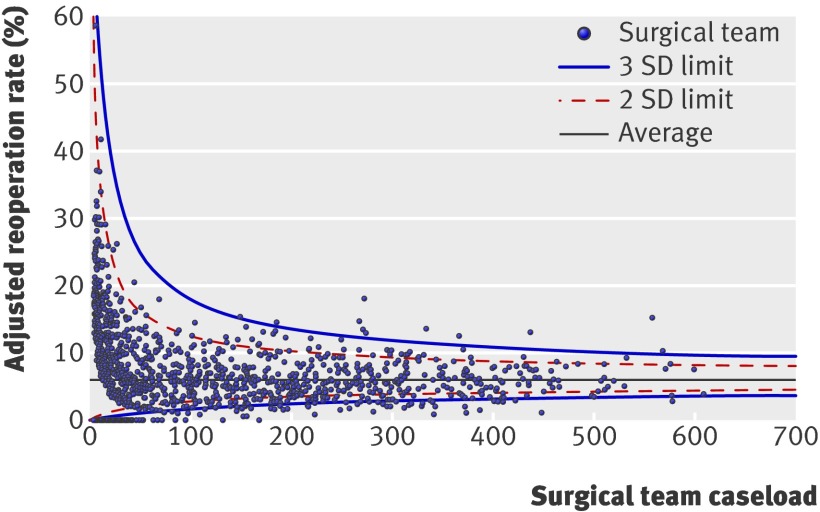
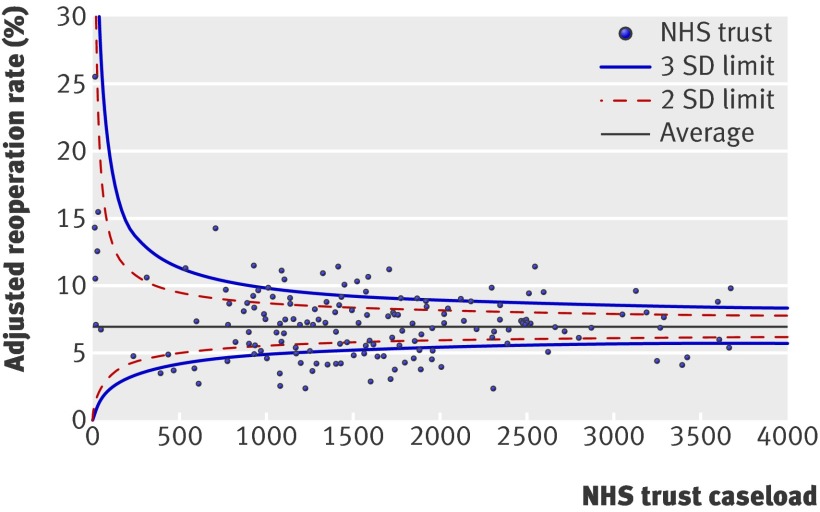
Results: The national reoperation rate was 6.5% (15,986/246,469). A large degree of variation was identified among institutions and surgeons. Even among institutions and surgical teams with high caseloads, threefold and fivefold differences in reoperation rates were observed between the highest and lowest performing trusts and surgeons. Of the NHS trusts studied, 14.1% (22/156) had adjusted reoperation rates above the upper 99.8% control limit. Factors independently associated with higher risk of reoperation were diagnosis of inflammatory bowel disease (odds ratio 1.33 (95% CI 1.24 to 1.42), P<0.001), presence of multiple comorbidity (odds ratio 1.34 (1.29 to 1.39), P<0.001), social deprivation (1.14 (1.08 to 1.20) for most deprived, P<0.001), male sex (1.33 (1.29 to 1.38), P<0.001), rectal resection (1.63 (1.56 to 1.71), P<0.001), laparoscopic surgery (1.11 (1.03 to 1.20), P = 0.006), and emergency admission (1.21 (1.17 to 1.26), P<0.001).
Conclusions: There is large variation in reoperation after colorectal surgery between hospitals and surgeons in England. If data accuracy can be assured, reoperation may allow performance to be checked against national standards from current routinely collected data, alongside other indicators such as mortality.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
Comment in
-
Measuring quality in colorectal surgery.BMJ. 2011 Aug 16;343:d4859. doi: 10.1136/bmj.d4859. BMJ. 2011. PMID: 21846715 No abstract available.
References
-
- Alves A, Panis Y, Mathieu P, Mantion G, Kwiatkowski F, Slim K. Postoperative mortality and morbidity in French patients undergoing colorectal surgery: results of a prospective multicenter study. Arch Surg 2005;140:278-83, discussion 84. - PubMed
-
- Faiz O, Brown T, Bottle A, Burns EM, Darzi AW, Aylin P. Impact of hospital institutional volume on postoperative mortality after major emergency colorectal surgery in English National Health Service Trusts, 2001 to 2005. Dis Colon Rectum 2010;53:393-401. - PubMed
-
- Morris E, Quirke P, Thomas JD, Fairley L, Cottier B, Forman D. Unacceptable variation in abdominoperineal excision rates for rectal cancer: time to intervene? Gut 2008;57:1690-7. - PubMed
-
- Morris EJ, Taylor EF, Thomas JD, Quirke P, Finan PJ, Coleman MP, et al. Thirty-day postoperative mortality after colorectal cancer surgery in England. Gut 2011;60:806-13. - PubMed