

Use of radioactive iodine for thyroid cancer
- PMID: 21846853
- PMCID: PMC3352591
- DOI: 10.1001/jama.2011.1139
Use of radioactive iodine for thyroid cancer
Abstract
Context: Substantial uncertainty persists about the indications for radioactive iodine for thyroid cancer. Use of radioactive iodine over time and the correlates of its use remain unknown.
Objective: To determine practice patterns, the degree to which hospitals vary in their use of radioactive iodine, and factors that contribute to this variation.
Design, setting, and patients: Time trend analysis of radioactive iodine use in a cohort of 189,219 patients with well-differentiated thyroid cancer treated at 981 hospitals associated with the US National Cancer Database between 1990 and 2008. We used multilevel analysis to assess the correlates of patient and hospital characteristics on radioactive iodine use in the cohort treated from 2004 to 2008.
Main outcome measure: Use of radioactive iodine after total thyroidectomy.
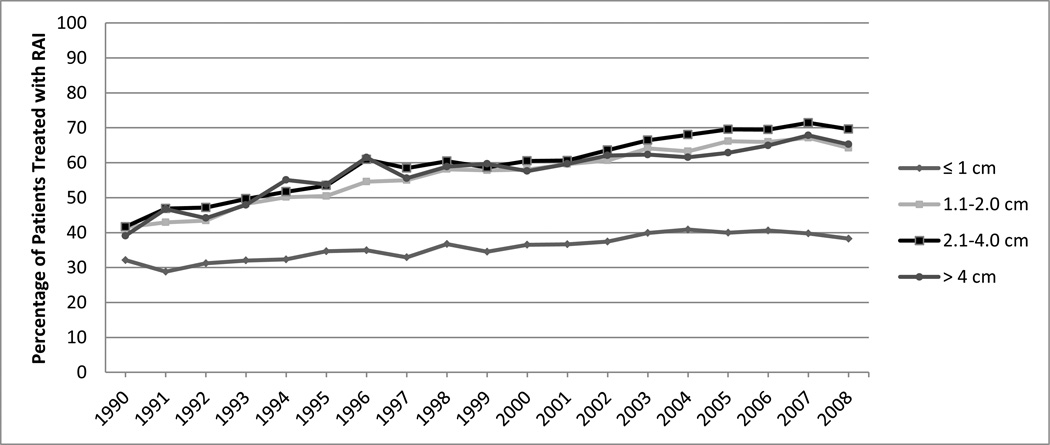
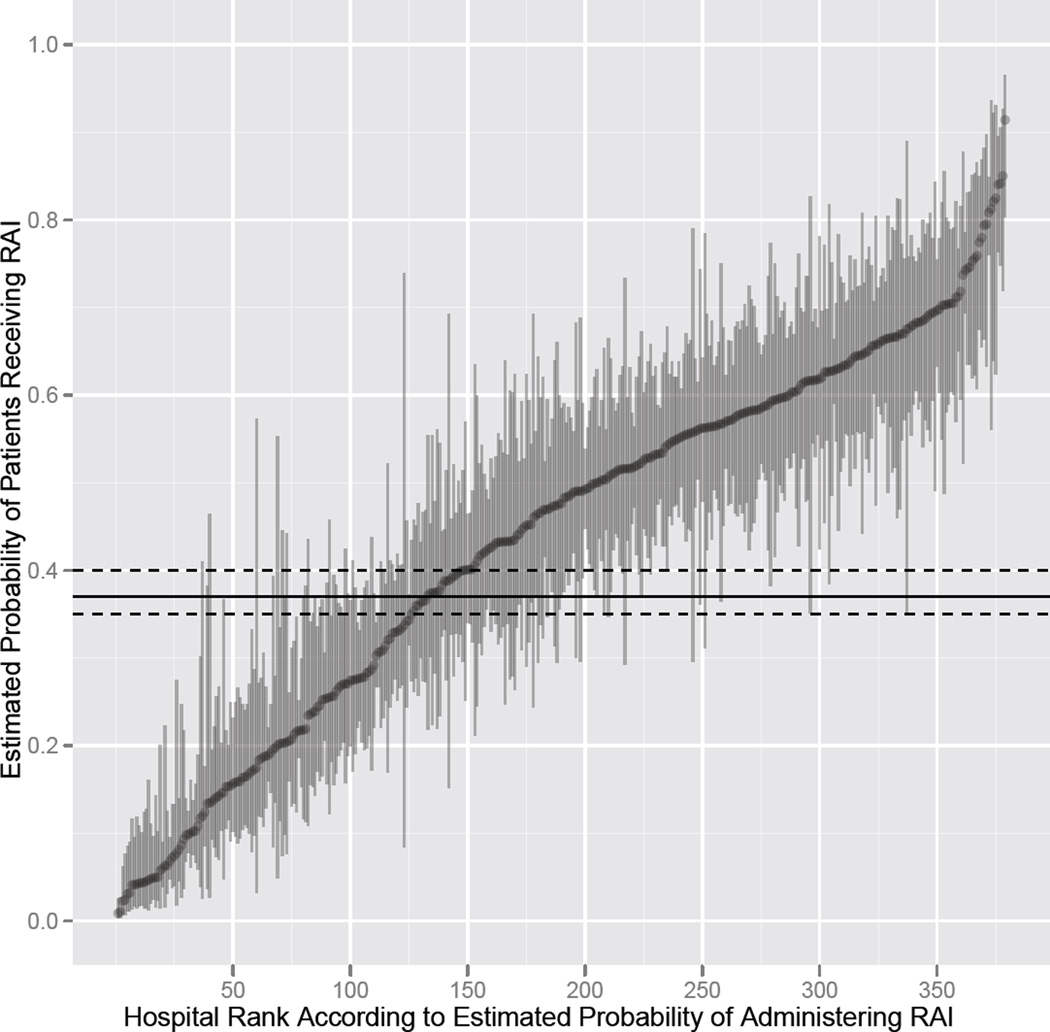
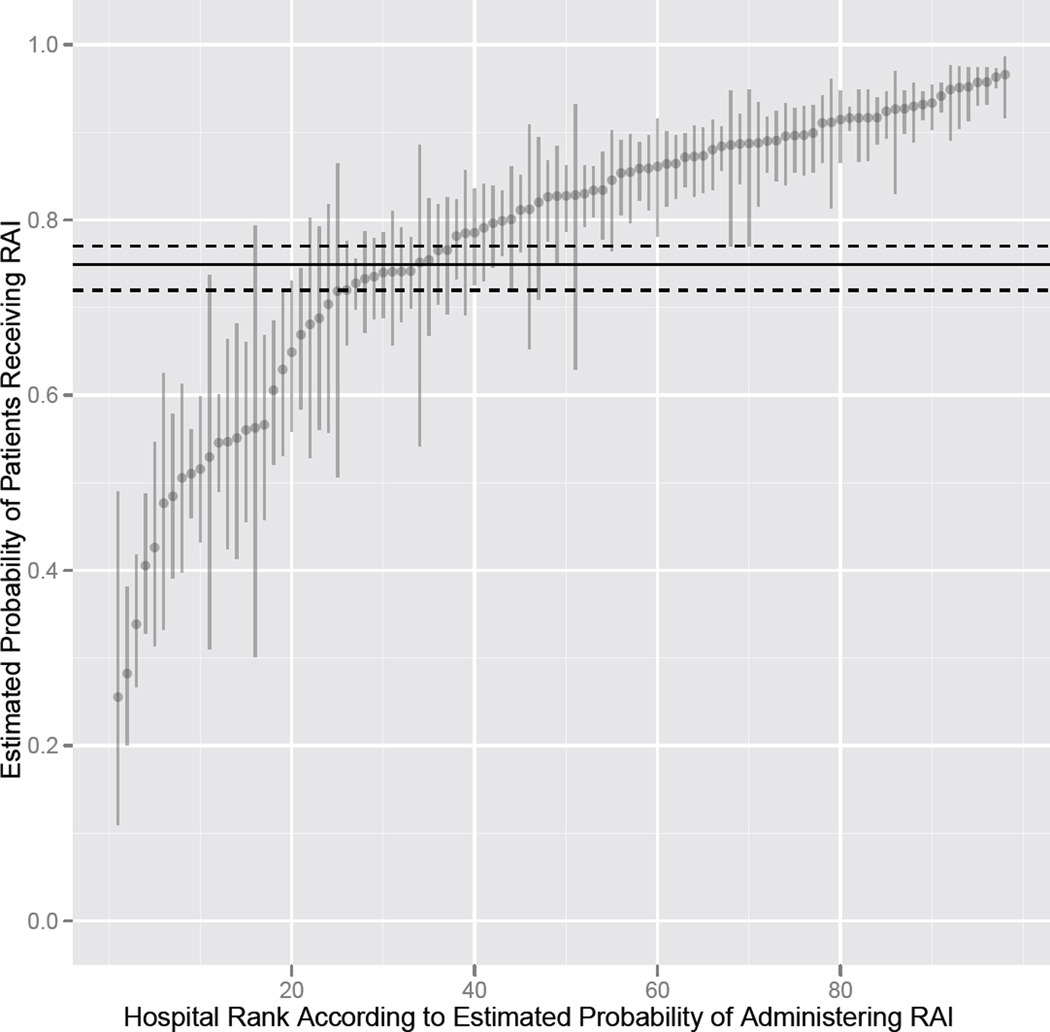
Results: Between 1990 and 2008, across all tumor sizes, there was a significant increase in the proportion of patients with well-differentiated thyroid cancer receiving radioactive iodine (1373/3397 [40.4%] vs 11,539/20,620 [56.0%]; P < .001). Multivariable analysis of patients treated from 2004 to 2008 found that there was a statistical difference in radioactive iodine use between American Joint Committee on Cancer stages I and IV (odds ratio [OR], 0.34; 95% confidence interval [CI], 0.31-0.37) but not between stages II/III and IV (for stage II vs stage IV, OR, 0.97; 95% CI, 0.88-1.07 and for stage III vs stage IV, OR, 1.06; 95% CI, 0.95-1.17). In addition to patient and tumor characteristics, hospital volume was associated with radioactive iodine use. Wide variation in radioactive iodine use existed, and only 21.1% of this variation was accounted for by patient and tumor characteristics. Hospital type and case volume accounted for 17.1% of the variation. After adjusting for available patient, tumor, and hospital characteristics, 29.1% of the variance was attributable to unexplained hospital characteristics.
Conclusion: Among patients treated for well-differentiated thyroid cancer at hospitals in the National Cancer Database, there was an increase in the proportion receiving radioactive iodine between 1990 and 2008; much of the variation in use was associated with hospital characteristics.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Comment in
-
The hazards of evidence-based medicine: assessing variations in care.JAMA. 2011 Aug 17;306(7):762-3. doi: 10.1001/jama.2011.1181. JAMA. 2011. PMID: 21846860 No abstract available.
References
-
- Varma VM, Beierwaltes WH, Nofal MM, Nishiyama RH, Copp JE. Treatment of thyroid cancer. Death rates after surgery and after surgery followed by sodium iodide I-131. JAMA. 1970 Nov 23;214(8):1437–1442. - PubMed
-
- Chow SM, Yau S, Kwan CK, Poon PC, Law SC. Local and regional control in patients with papillary thyroid carcinoma: specific indications of external radiotherapy and radioactive iodine according to T and N categories in AJCC 6th edition. Endocr Relat Cancer. 2006 Dec;13(4):1159–1172. - PubMed
-
- Jung TS, Kim TY, Kim KW, et al. Clinical features and prognostic factors for survival in patients with poorly differentiated thyroid carcinoma and comparison to the patients with the aggressive variants of papillary thyroid carcinoma. Endocr J. 2007 Apr;54(2):265–274. - PubMed
-
- Podnos YD, Smith DD, Wagman LD, Ellenhorn JD. Survival in patients with papillary thyroid cancer is not affected by the use of radioactive isotope. J Surg Oncol. 2007 Jul 1;96(1):3–7. - PubMed
-
- Jonklaas J, Sarlis NJ, Litofsky D, et al. Outcomes of patients with differentiated thyroid carcinoma following initial therapy. Thyroid. 2006 Dec;16(12):1229–1242. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
