

Closed platysmotomy: a new procedure for the treatment of platysma bands without skin dissection
- PMID: 21847680
- PMCID: PMC3192284
- DOI: 10.1007/s00266-011-9782-0
Closed platysmotomy: a new procedure for the treatment of platysma bands without skin dissection
Abstract
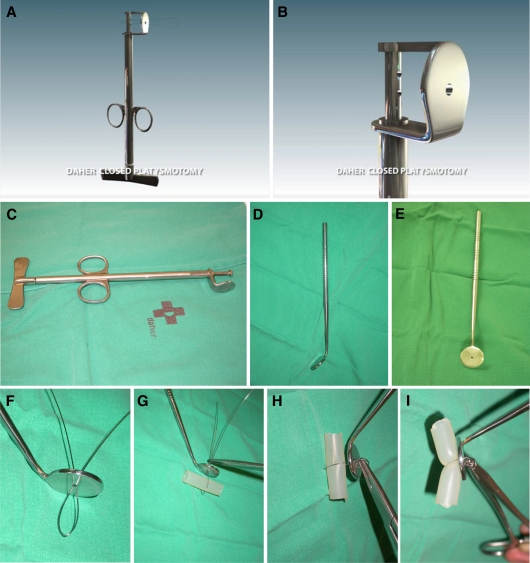
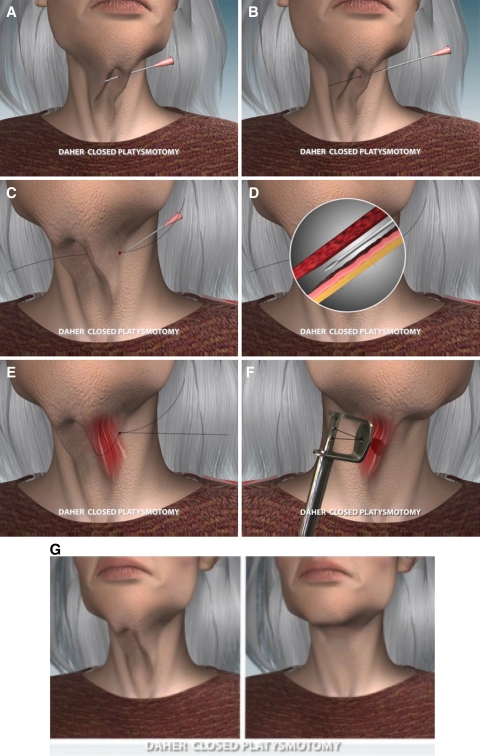
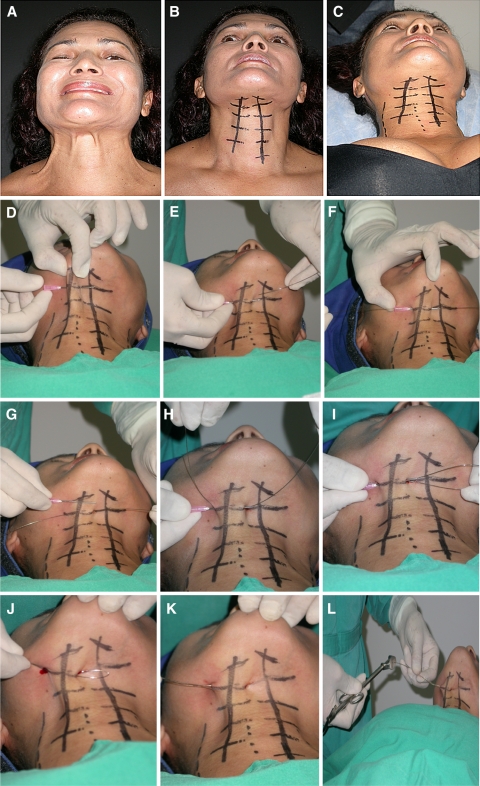
Platysma muscular bands are present during the aging period, generally starting in the second half of the fourth decade of life in both sexes. One or two bands along the anterior segment of the neck are the most frequent, with varied extensions and appearances. The literature records different techniques for solving the problem of platysma bands. All the methods involve submental incision, cutaneous dissection, and various tactics for eliminating the action of the platysma bands. This report aims to describe a procedure for deactivating these bands using a percutaneous approach that eliminates the need for submental, cutaneous incision and dissection. This technique involves the use of a steel wire loop that encircles the platysma band and is connected to a device known as the platysmotome through two puncture holes in the skin. Three to six sections along each band eliminate the platysma band, leaving no visible marks on the skin. This method is indicated as an isolated procedure for patients with visible platysma bands and no skin flaccidity, patients with recurring bands after face-lifting and no cervical skin flaccidity, patients who have bands with little cervical skin flaccidity but do not care to undergo face-lifting, and patients who undergo face-lifts for platysma bands that include closed platysmotomy and tightening of the platysma by lateral suture. The described technique is a method specifically designed for deactivation of the platysma bands that can be used both in isolation and in conjunction with face-lifting. Because this method avoids submental, cervical incision and dissection, it is a less invasive technique for "deleting" the bands, whether applied alone or in association with face-lifting. From May 2008 to November 2009 (19 months), 61 patients underwent surgery for the correction of platysma bands via percutaneous myotomy. Among them, the first 11 patients received postoperative follow-up evaluation ranging from 8 to 17 months.
Figures






Comment in
-
Closed platysmotomy: a new procedure to treat platysma bands.Aesthetic Plast Surg. 2013 Jun;37(3):636-7. doi: 10.1007/s00266-012-0037-5. Epub 2013 Apr 3. Aesthetic Plast Surg. 2013. PMID: 23549861 No abstract available.
Similar articles
-
Composite platysmaplasty and closed percutaneous platysma myotomy: a simple way to treat deformities of the neck caused by aging.Aesthet Surg J. 2009 Sep-Oct;29(5):344-54. doi: 10.1016/j.asj.2009.04.007. Aesthet Surg J. 2009. PMID: 19825461
-
Closed platysmotomy: a new procedure to treat platysma bands.Aesthetic Plast Surg. 2013 Jun;37(3):636-7. doi: 10.1007/s00266-012-0037-5. Epub 2013 Apr 3. Aesthetic Plast Surg. 2013. PMID: 23549861 No abstract available.
-
Isolated neck-lifting procedure: isolated stork lift.Aesthetic Plast Surg. 2013 Apr;37(2):205-9. doi: 10.1007/s00266-012-0002-3. Epub 2013 Jan 10. Aesthetic Plast Surg. 2013. PMID: 23307054
-
Surgical Management of Platysma Bands: A Narrative Review of Evolving Concepts and Changing Techniques for Neck Rejuvenation.Aesthetic Plast Surg. 2023 Oct;47(5):1824-1834. doi: 10.1007/s00266-023-03604-8. Epub 2023 Aug 31. Aesthetic Plast Surg. 2023. PMID: 37653178 Review.
-
Lateral Skin-Platysma Displacement: A New Approach to Neck Rejuvenation Through a Lateral Approach.Clin Plast Surg. 2019 Oct;46(4):587-602. doi: 10.1016/j.cps.2019.06.006. Epub 2019 Aug 6. Clin Plast Surg. 2019. PMID: 31514810 Review.
Cited by
-
Efficacy and Safety of OnabotulinumtoxinA for the Treatment of Platysma Prominence: A Randomized Phase 2 Dose-Ranging Study.Plast Reconstr Surg. 2025 Jan 1;155(1):79-88. doi: 10.1097/PRS.0000000000011472. Epub 2024 Apr 16. Plast Reconstr Surg. 2025. PMID: 38640068 Free PMC article. Clinical Trial.
-
Investigating the Contraction Pattern of the Zygomaticus Major Muscle and its Clinical Relevance: A Functional MRI Study.Aesthetic Plast Surg. 2024 Jul;48(14):2722-2729. doi: 10.1007/s00266-024-03876-8. Epub 2024 Feb 27. Aesthetic Plast Surg. 2024. PMID: 38413445 Free PMC article.
-
Platysma Prominence: Review and Expert Analysis of Clinical Presentation, Burden, and Treatment Considerations.Plast Reconstr Surg Glob Open. 2025 Feb 5;13(2):e6490. doi: 10.1097/GOX.0000000000006490. eCollection 2025 Feb. Plast Reconstr Surg Glob Open. 2025. PMID: 39911534 Free PMC article.
-
Horizontal necklines correction with absorbable braided polydioxanone threads: Case series.Skin Res Technol. 2024 Mar;30(3):e13617. doi: 10.1111/srt.13617. Skin Res Technol. 2024. Retraction in: Skin Res Technol. 2025 Jun;31(6):e70186. doi: 10.1111/srt.70186. PMID: 38444188 Free PMC article. Retracted.
-
Improving Neck and Jawline Aesthetics With OnabotulinumtoxinA by Minimizing Platysma Muscle Contraction Effects: Efficacy and Safety Results in a Phase 3 Randomized, Placebo-Controlled Study.Aesthet Surg J. 2025 Jan 16;45(2):194-201. doi: 10.1093/asj/sjae220. Aesthet Surg J. 2025. PMID: 39475141 Free PMC article. Clinical Trial.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
