

Efficacy of dosimetric versus empiric prescribed activity of 131I for therapy of differentiated thyroid cancer
- PMID: 21849530
- PMCID: PMC7372577
- DOI: 10.1210/jc.2011-0494
Efficacy of dosimetric versus empiric prescribed activity of 131I for therapy of differentiated thyroid cancer
Abstract
Background: The optimal management of high-risk patients with differentiated thyroid cancer (DTC) consists of thyroidectomy followed by radioiodine ((131)I) therapy. The prescribed activity of (131)I can be determined using two approaches: 1) empiric prescribed activity of (131)I (E-Rx); and 2) dosimetry-based prescribed activity of (131)I (D-Rx).
Aim: The aim of the study was to compare the relative treatment efficacy and side effects of D-Rx vs. E-Rx.
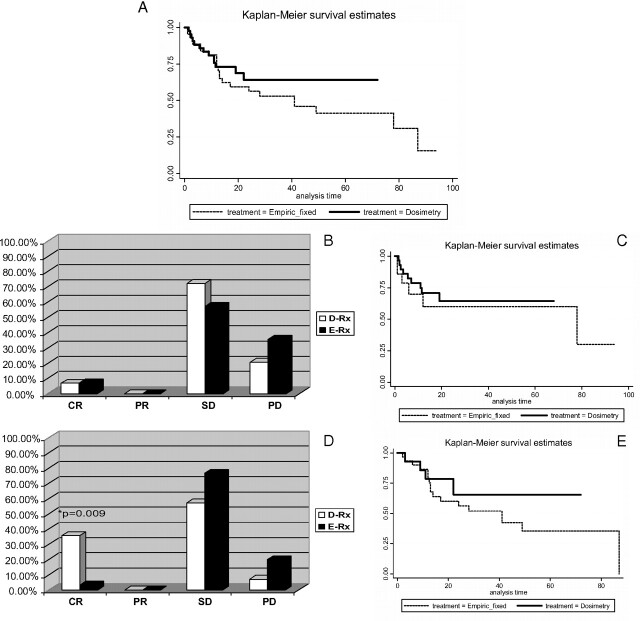
Methods: A retrospective analysis was performed of patients with distant metastases and/or locoregionally advanced radioiodine-avid DTC who were treated with either D-Rx or E-Rx. Response to treatment was based on RECIST (Response Evaluation Criteria in Solid Tumors) 1.1 criteria.
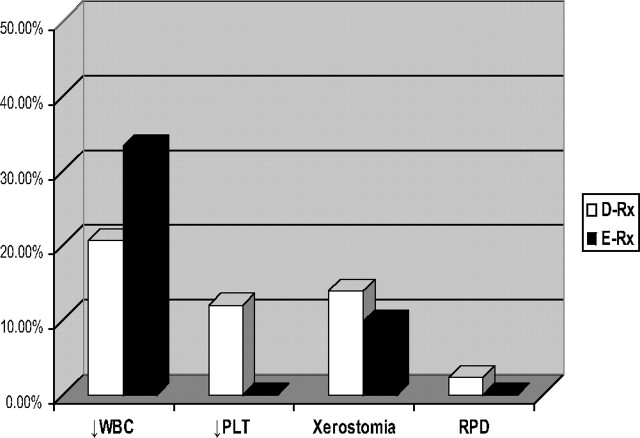
Results: The study group consisted of 87 patients followed for 51 ± 35 months, of whom 43 were treated with D-Rx and 44 with E-Rx. Multivariate analysis, controlling for age, gender, and status of metastases revealed that the D-Rx group tended to be 70% less likely to progress (odds ratio, 0.29; 95% confidence interval, 0.087-1.02; P = 0.052) and more likely to obtain complete response (CR) compared to the E-Rx group (odds ratio, 8.2; 95% confidence interval, 1.2-53.5; P = 0.029). There was an association in the D-Rx group between the observed CR and percentage of maximum tolerable activity given as a first treatment of (131)I (P = 0.030). The advantage of D-Rx was specifically apparent in the locoregionally advanced group because CR was significantly higher in D-Rx vs. E-Rx in this group of patients (35.7 vs. 3.3%; P = 0.009). The rates of partial response, stable disease, and progression-free survival, as well as the frequency of side effects, were not significantly different between the two groups.
Conclusion: Higher efficacy of D-Rx with a similar safety profile compared to E-Rx supports the rationale for employing individually prescribed activity in high-risk patients with DTC.
Figures
Comment in
-
The "reset button" revisited: why high activity 131I therapy of advanced differentiated thyroid cancer after dosimetry is advantageous for patients.Eur J Nucl Med Mol Imaging. 2017 Jun;44(6):915-917. doi: 10.1007/s00259-017-3649-9. Epub 2017 Feb 16. Eur J Nucl Med Mol Imaging. 2017. PMID: 28210770 No abstract available.
References
-
- Jemal A , Siegel R , Xu J , Ward E. 2010. Cancer statistics 2010. CA Cancer J Clin 60:277–300 - PubMed
-
- Davies L , Welch HG. 2006. Increasing incidence of thyroid cancer in the United States, 1988–2005. JAMA 295:2164–2167 - PubMed
-
- Ries LA , Eisner MP , Kosary CL. 2006. SEER cancer statistics review, 1975–2000/2003. Bethesda, MD: National Cancer Institute; seer.cancer.gov/csr/1975_2001/
-
- Chen AY , Jemal A , Ward EM. 2009. Increasing incidence of differentiated thyroid cancer in the United States, 1988–2005. Cancer 115:3801–3807 - PubMed
-
- Rego-Iraeta A , Pérez-Méndez LF , Mantinan B , Garcia-Mayor RV. 2009. Time trends for thyroid cancer in northwestern Spain: true rise in the incidence of micro and larger forms of papillary thyroid cancer. Thyroid 19:333–340 - PubMed
