

Systemic infections mimicking thrombotic thrombocytopenic purpura
- PMID: 21850657
- PMCID: PMC3420338
- DOI: 10.1002/ajh.22091
Systemic infections mimicking thrombotic thrombocytopenic purpura
Abstract
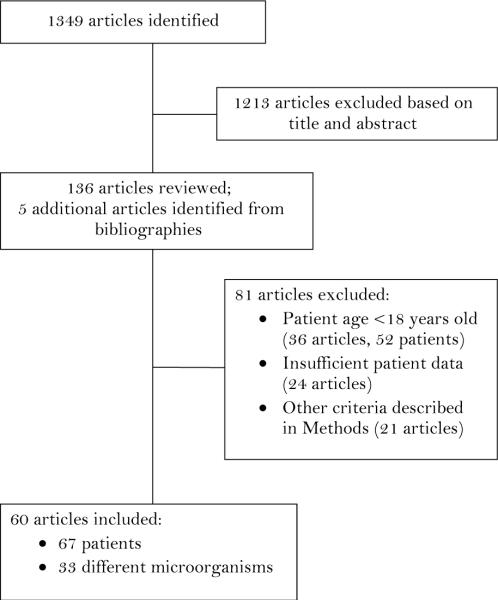
The absence of specific diagnostic criteria, the urgency to begin plasma exchange treatment, and the risk for complications from plasma exchange make the initial evaluation of patients with suspected thrombotic thrombocytopenic purpura (TTP) difficult. Systemic infections may mimic the presenting clinical features of TTP. In the Oklahoma TTP-HUS (hemolytic-uremic syndrome) Registry, 1989-2010, 415 consecutive patients have been clinically diagnosed with their first episode of TTP; in 31 (7%) the presenting clinical features were subsequently attributed to a systemic infection. All 31 patients had diagnostic criteria for TTP; 16 (52%) had the complete "pentad" of microangiopathic hemolytic anemia, thrombocytopenia, neurologic abnormalities, renal failure, and fever. Four (16%) of 25 patients who had ADAMTS13 measurements had <10% activity; three patients had a demonstrable ADAMTS13 inhibitor. Compared with 62 patients with severe ADAMTS13 deficiency (<10%) who had no recognized alternative disorders, patients with systemic infections had more frequent fever, coma, renal failure, and the complete "pentad" of clinical features. Seventeen different infectious etiologies were documented. A systematic literature review identified 67 additional patients with a diagnosis of TTP or HUS and also a systemic infection. Among all 98 patients, infections with 41 different bacteria, viruses, and fungi were documented, suggesting that many different systemic infections may mimic the presenting clinical features of TTP. Initial plasma exchange treatment is appropriate in critically ill patients with diagnostic features of TTP, even if a systemic infection is suspected. Continuing evaluation to document a systemic infection is essential to determine the appropriateness of continued plasma exchange.
Copyright © 2011 Wiley-Liss, Inc.
Figures
References
-
- Amorosi EL, Ultmann JE. Thrombotic thrombocytopenic purpura: report of 16 cases and review of the literature. Medicine. 1966;45:139–59.
-
- Rock GA, Shumak KH, Buskard NA, Blanchette VS, Kelton JG, Nair RC, et al. Comparison of plasma exchange with plasma infusion in the treatment of thrombotic thrombocytopenic purpura. New Eng J Med. 1991;325:393–97. - PubMed
-
- George JN. How I treat patients with thrombotic thrombocytopenic purpura - 2010. Blood. 2010;116:4060–4069. - PubMed
-
- Clark WF, Garg AX, Blake PG, Rock GA, Heidenhwim AP, Sackett DL. Effect of awareness of a randomized controlled trial on use of experimental therapy. JAMA. 2003;290:1351–55. - PubMed
-
- Brain MC, Dacie JV, Hourihane OB. Microangiopathic hemolytic anemia: the possible role of vascular lesions in pathogenesis. Br J Haematol. 1962;8:358–74. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical