

Topical capsaicin for pain management: therapeutic potential and mechanisms of action of the new high-concentration capsaicin 8% patch
- PMID: 21852280
- PMCID: PMC3169333
- DOI: 10.1093/bja/aer260
Topical capsaicin for pain management: therapeutic potential and mechanisms of action of the new high-concentration capsaicin 8% patch
Abstract
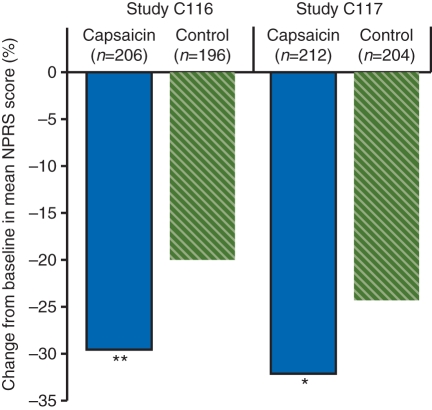
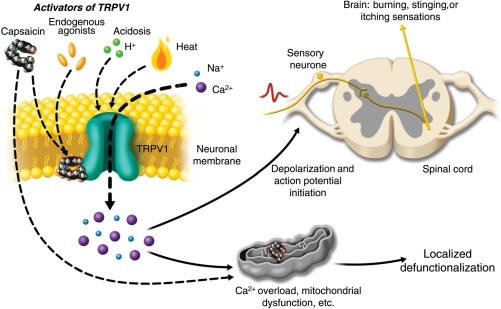
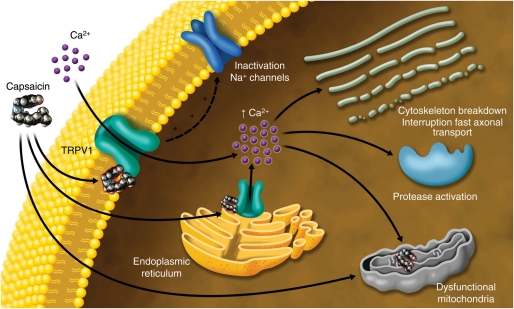
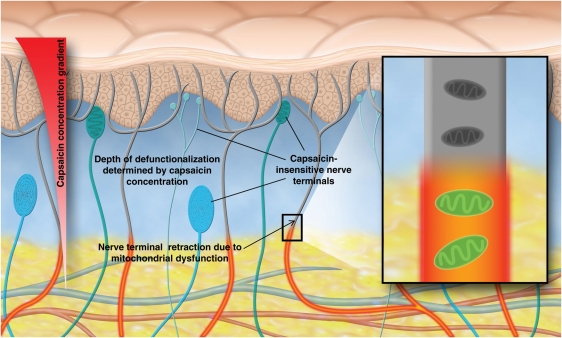
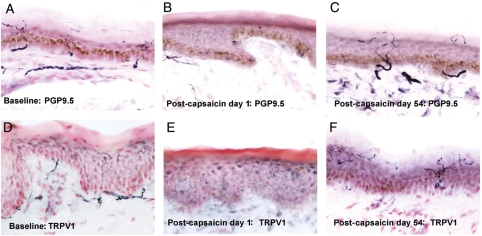
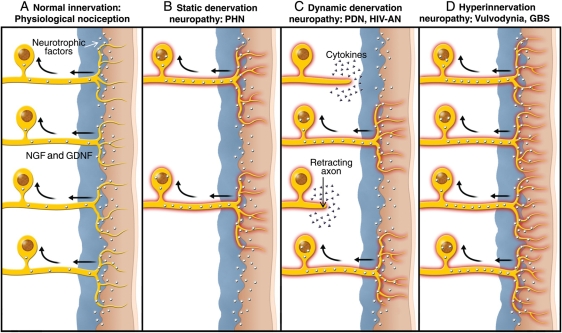
Topical capsaicin formulations are used for pain management. Safety and modest efficacy of low-concentration capsaicin formulations, which require repeated daily self-administration, are supported by meta-analyses of numerous studies. A high-concentration capsaicin 8% patch (Qutenza™) was recently approved in the EU and USA. A single 60-min application in patients with neuropathic pain produced effective pain relief for up to 12 weeks. Advantages of the high-concentration capsaicin patch include longer duration of effect, patient compliance, and low risk for systemic effects or drug-drug interactions. The mechanism of action of topical capsaicin has been ascribed to depletion of substance P. However, experimental and clinical studies show that depletion of substance P from nociceptors is only a correlate of capsaicin treatment and has little, if any, causative role in pain relief. Rather, topical capsaicin acts in the skin to attenuate cutaneous hypersensitivity and reduce pain by a process best described as 'defunctionalization' of nociceptor fibres. Defunctionalization is due to a number of effects that include temporary loss of membrane potential, inability to transport neurotrophic factors leading to altered phenotype, and reversible retraction of epidermal and dermal nerve fibre terminals. Peripheral neuropathic hypersensitivity is mediated by diverse mechanisms, including altered expression of the capsaicin receptor TRPV1 or other key ion channels in affected or intact adjacent peripheral nociceptive nerve fibres, aberrant re-innervation, and collateral sprouting, all of which are defunctionalized by topical capsaicin. Evidence suggests that the utility of topical capsaicin may extend beyond painful peripheral neuropathies.
Figures
References
-
- Szallasi A, Blumberg PM. Vanilloid (capsaicin) receptors and mechanisms. Pharmacol Rev. 1999;51:159–212. - PubMed
-
- Turnbull A. Tincture of capsaicin as a remedy for chilblains and toothache. Dublin Free Press. 1850;1:95–6.
-
- Hempenstall K, Nurmikko TJ, Johnson RW, A'Hern RP, Rice AS. Analgesic therapy in postherpetic neuralgia: a quantitative systematic review. PLoS Med. 2005;2:e164. doi:10.1371/journal.pmed.0020164. - DOI - PMC - PubMed
-
- Altman R, Barkin RL. Topical therapy for osteoarthritis: clinical and pharmacologic perspectives. Postgrad Med. 2009;121:139–47. doi:10.3810/pgm.2009.03.1986. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
