

Arm exercise stress perfusion imaging predicts clinical outcome
- PMID: 21852405
- PMCID: PMC3233885
- DOI: 10.1152/japplphysiol.00725.2011
Arm exercise stress perfusion imaging predicts clinical outcome
Abstract
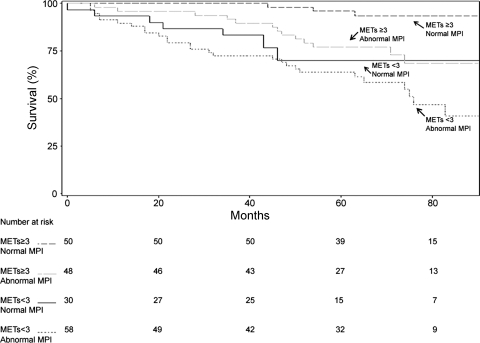
Treadmill exercise capacity in resting metabolic equivalents (METs) and stress hemodynamic, electrocardiographic (ECG), and myocardial perfusion imaging (MPI) responses are independently predictive of adverse clinical events. However, limited data exist for arm ergometer stress testing (AXT) in patients who cannot perform leg exercise because of lower extremity disabilities. We sought to determine the extent to which AXT METs, hemodynamic, ECG, and MPI responses to arm exercise add independent incremental value to demographic and clinical variables for prediction of all-cause mortality, myocardial infarction (MI), or late coronary revascularization, individually or as a composite. A prospective cohort of 186 patients aged 64 ± 10 (SD) yr, unable to perform lower extremity exercise, underwent AXT MPI for clinical reasons between 1997 and 2002, and were followed for 62 ± 23 mo, to an endpoint of death or 12/31/2006. Average annual rates were 5.4% for mortality, 2.2% for MI, 2.5% for late coronary revascularization, and 8.0% for combined events. After adjustment for age and clinical variables, AXT METs [P < 0.05; hazard ratio (HR) = 0.59; confidence interval (CI) = 0.35-0.84] and abnormal MPI (P < 0.01; HR = 2.48; CI = 2.15-2.81) were independently predictive of mortality. A positive AXT ECG (P < 0.05; HR = 2.61; CI = 2.13-3.10) was predictive of MI. Death and MI combined were prognosticated by METs (P < 0.05; HR = 0.63; CI = 0.41-0.85), MPI (P < 0.05; HR = 1.77; CI = 1.49-2.05), and a positive AXT ECG (P < 0.05; HR = 1.86; CI = 1.55-2.17). In conclusion, for high risk older patients who cannot perform leg exercise because of lower extremity disabilities, AXT METs are as important as MPI for prediction of mortality alone and death and MI combined, and a positive AXT ECG prognosticates MI alone and death and MI combined.
Figures



Comment in
-
Exercise testing and disease risk: individualized medicine without the "omics"?J Appl Physiol (1985). 2011 Dec;111(6):1539. doi: 10.1152/japplphysiol.01154.2011. Epub 2011 Sep 22. J Appl Physiol (1985). 2011. PMID: 21940848 No abstract available.
References
-
- Astrand PO, Rodahl K. Textbook of Work Physiology (3rd ed.). New York: McGraw-Hill, 1986, chapt. 8, p. 365
-
- Astrand PO, Saltin B. Maximal oxygen uptake and heart rate in various types of muscular activity. J Appl Physiol 16: 977–981, 1961 - PubMed
-
- Balady GJ, Weiner DA, Rothendler JA, Ryan TJ. (with the technical assistance of Mangene C, LaGambina J, McCarthy C.). Arm exercise-thallium imaging testing for the detection of coronary artery disease. J Am Coll Cardiol 9: 84–88, 1987 - PubMed
-
- Berman DS, Kang X, Van Train KF, Lewin HC, Cohen I, Areeda J, Friedman JD, Germano G, Shaw LJ, Hachamovitch R. Comparative value of automatic quantitative analysis vs. semi-quantitative visual analysis of exercise myocardial perfusion single-photon emission computed tomography. J Am Coll Cardiol 32: 1987–1995, 1998 - PubMed
-
- Blair SN, Kohl HW, 3rd, Paffenbarger RS, Jr, Clark DG, Cooper KH, Gibbons LW. Physical fitness and all-cause mortality: a prospective study of healthy men and women. JAMA 262: 2395–2401, 1989 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources