

Neonatal abstinence syndrome: transitioning methadone-treated infants from an inpatient to an outpatient setting
- PMID: 21852772
- PMCID: PMC3682112
- DOI: 10.1038/jp.2011.114
Neonatal abstinence syndrome: transitioning methadone-treated infants from an inpatient to an outpatient setting
Abstract
Objective: Each year in the US ∼50 000 neonates receive inpatient pharmacotherapy for the treatment of neonatal abstinence syndrome (NAS). The objective of this study is to compare the safety and efficacy of a traditional inpatient only approach with a combined inpatient and outpatient methadone treatment program.
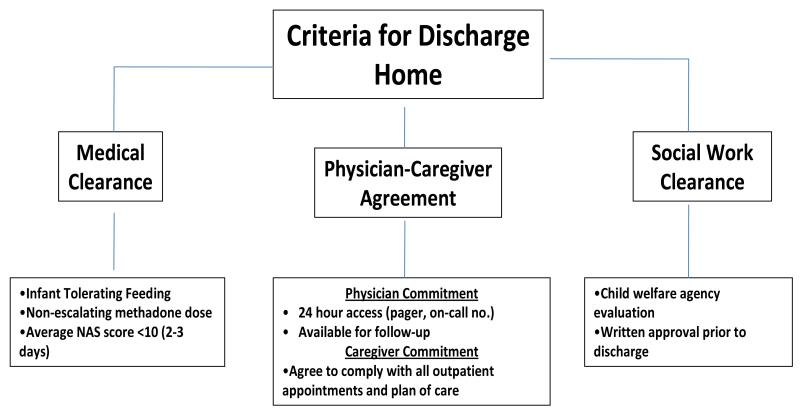
Study design: Retrospective review (2007 to 2009). Infants were born to mothers maintained on methadone in an antenatal substance abuse program. All infants received methadone for NAS treatment as inpatient. Methadone weaning for the traditional group (75 patients) was inpatient, whereas the combined group (46 patients) was outpatient.
Result: Infants in the traditional and combined groups were similar in demographics, obstetrical risk factors, birth weight, gestational age (GA) and the incidence of prematurity (34 and 31%). Hospital stay was shorter in the combined than in the traditional group (13 vs 25 days; P<0.01). Although the duration of treatment was longer for infants in the combined group (37 vs 21 days, P<0.01), the cumulative methadone dose was similar (3.6 vs 3.1 mg kg(-1), P=0.42). Follow-up information (at least 3 months) was available for 80% of infants in the traditional and 100% of infants in the combined group. All infants in the combined group were seen ≤72 h from hospital discharge. Breastfeeding was more common among infants in the combined group (24 vs 8% P<0.05). Following discharge there were no differences between the two groups in hospital readmissions for NAS. Prematurity (34 to 36 weeks GA) was the only predictor for hospital readmission for NAS in both groups (P=0.02, OR 5). Average hospital cost for each infant in the combined group was $13 817 less than in the traditional group.
Conclusion: A combined inpatient and outpatient methadone treatment in the management of NAS decreases hospital stay and substantially reduces cost. Additional studies are needed to evaluate the potential long-term benefits of the combined approach on infants and their families.
Figures
References
-
- Kuschel C. Managing drug withdrawal in the newborn infant. Semin Fetal Neonatal Med. 2007;12:127–33. - PubMed
-
- Finnegan LP, Connaughton JF, Jr, Kron RE, Emich JP. Neonatal abstinence syndrome: assessment and management. Addict Dis. 1975;2:141–58. - PubMed
-
- American Academy of Pediatrics (AAP) Committee on Drugs Neonatal Drug Withdrawal. Pediatrics. 1998;101:1079–88. - PubMed
-
- Ebner N, Rohrmeister K, Winklbaur B, Baewert A, Jagsch R, Peternell A, et al. Management of neonatal abstinence syndrome in neonates born to opioid maintained women. Drug Alcohol Depend. 2007;87:131–38. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
