

MRI findings of rectal submucosal tumors
- PMID: 21852910
- PMCID: PMC3150677
- DOI: 10.3348/kjr.2011.12.4.487
MRI findings of rectal submucosal tumors
Abstract
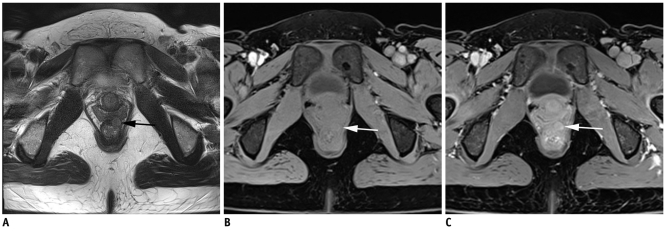
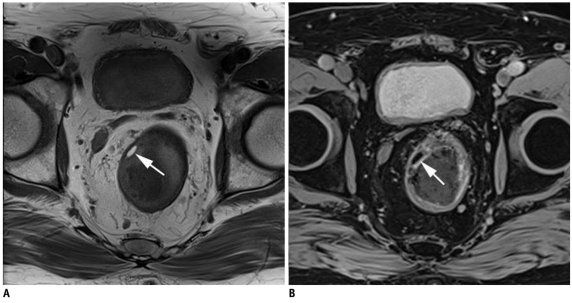
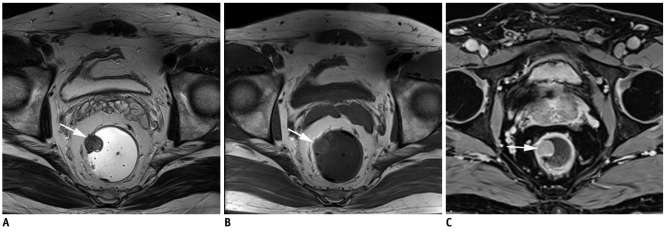
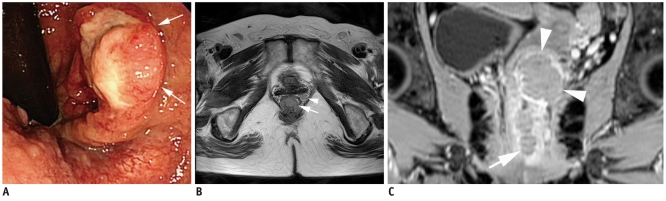
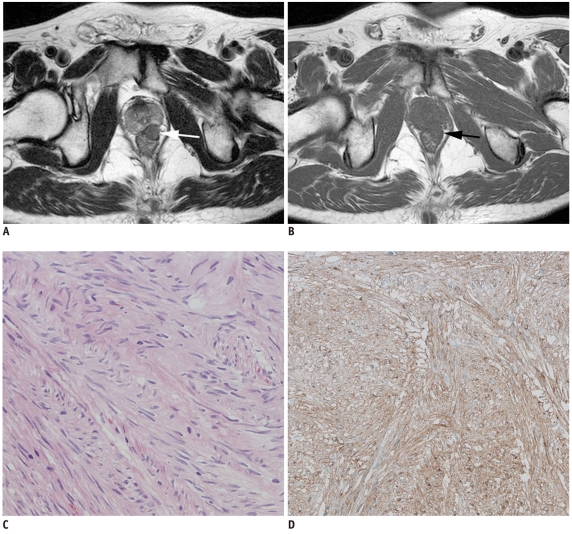
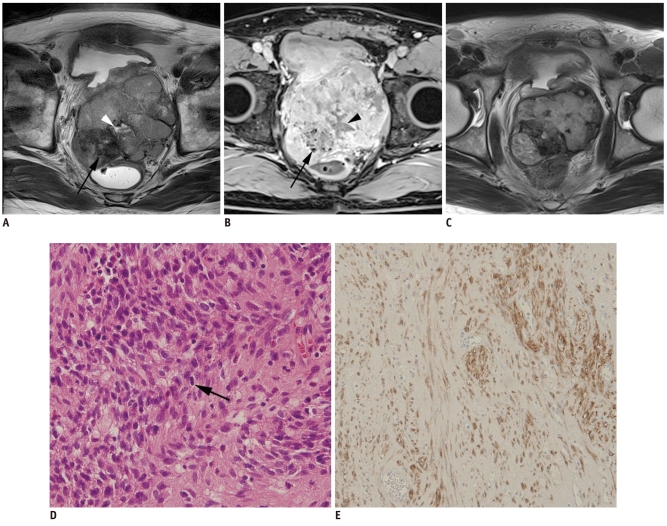
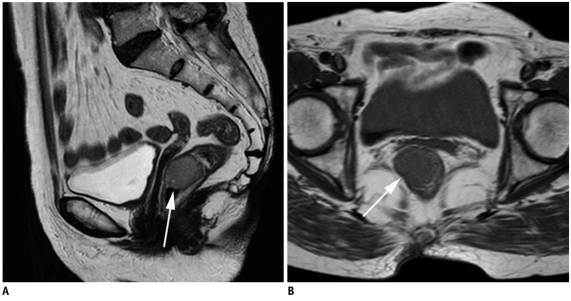
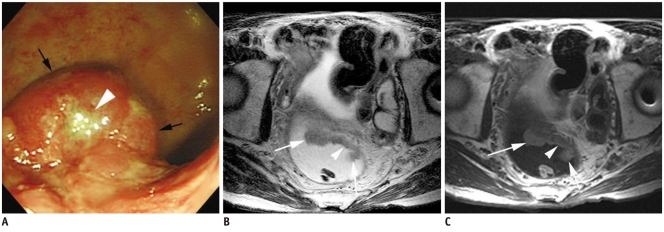
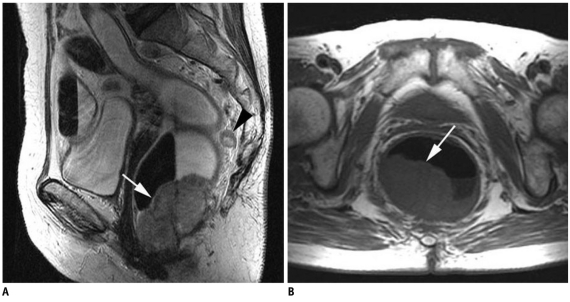
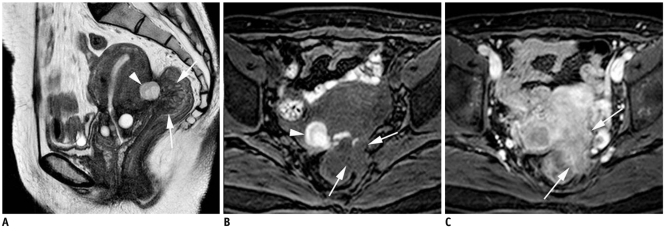
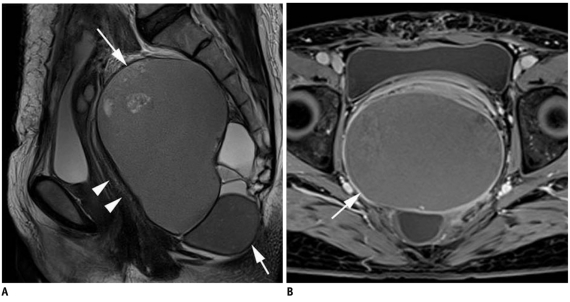
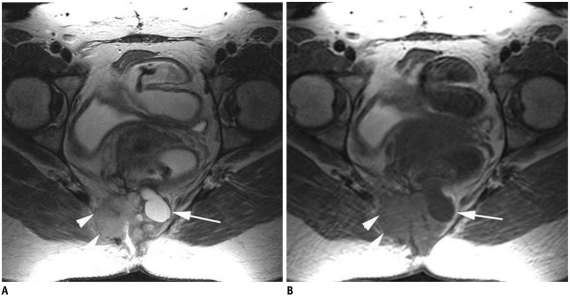
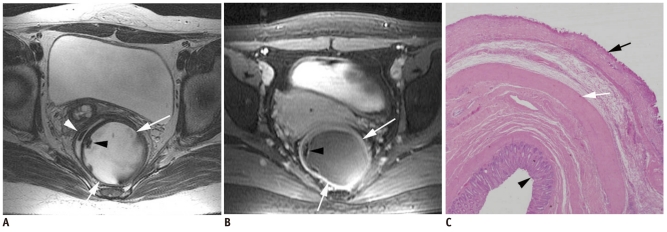
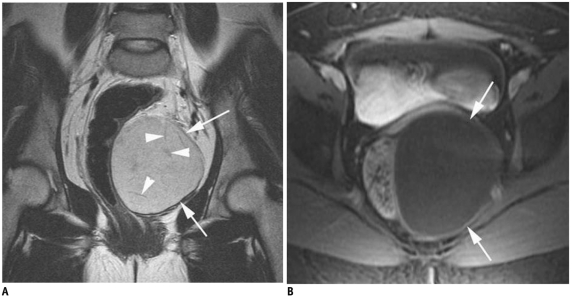
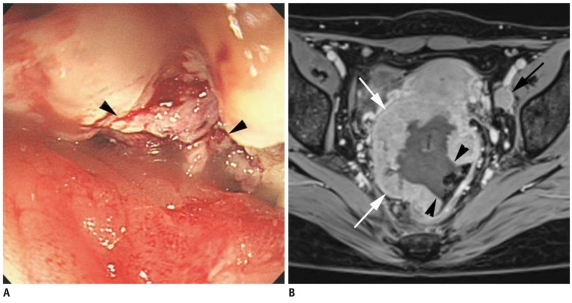
Rectal submucosal lesions encompass a wide variety of benign and malignant tumors involving the rectum. With optical colonoscopy, any mass-like protrusion covered by normal mucosa, whether the underlying process is intramural or extramural in origin, may be reported as a submucosal lesion. Whereas the assessment of submucosal lesions may be limited with performing optical colonoscopy, cross-sectional imaging such as CT, transrectal ultrasonography and MRI allows the evaluation of perirectal tissues and pelvic organs in addition to the entire thickness of the rectum, and so this is advantageous for the assessment of rectal submucosal tumors. Among these, MRI is the best investigative modality for soft tissue characterization. Therefore, knowledge of the MRI features of rectal submucosal tumors can help achieve accurate preoperative diagnoses and facilitate the appropriate management.
Keywords: MRI; Rectal cancer; Rectal submucosal tumor.
Figures
References
-
- Pickhardt PJ, Kim DH, Menias CO, Gopal DV, Arluk GM, Heise CP. Evaluation of submucosal lesions of the large intestine: part 1. Neoplasms. Radiographics. 2007;27:1681–1692. - PubMed
-
- Pickhardt PJ, Kim DH, Menias CO, Gopal DV, Arluk GM, Heise CP. Evaluation of submucosal lesions of the large intestine: part 2. Nonneoplastic causes. Radiographics. 2007;27:1693–1703. - PubMed
-
- Rouse HC, Godoy MC, Lee WK, Phang PT, Brown CJ, Brown JA. Imaging findings of unusual anorectal and perirectal pathology: a multi-modality approach. Clin Radiol. 2008;63:1350–1360. - PubMed
-
- Kloppel G, Perren A, Heitz PU. The gastroenteropancreatic neuroendocrine cell system and its tumors: the WHO classification. Ann N Y Acad Sci. 2004;1014:13–27. - PubMed
-
- Okamoto Y, Fujii M, Tateiwa S, Sakai T, Ochi F, Sugano M, et al. Treatment of multiple rectal carcinoids by endoscopic mucosal resection using a device for esophageal variceal ligation. Endoscopy. 2004;36:469–470. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
