

Comparative brain stem lesions on MRI of acute disseminated encephalomyelitis, neuromyelitis optica, and multiple sclerosis
- PMID: 21853047
- PMCID: PMC3154259
- DOI: 10.1371/journal.pone.0022766
Comparative brain stem lesions on MRI of acute disseminated encephalomyelitis, neuromyelitis optica, and multiple sclerosis
Abstract
Background: Brain stem lesions are common in patients with acute disseminated encephalomyelitis (ADEM), neuromyelitis optica (NMO), and multiple sclerosis (MS).
Objectives: To investigate comparative brain stem lesions on magnetic resonance imaging (MRI) among adult patients with ADEM, NMO, and MS.
Methods: Sixty-five adult patients with ADEM (n = 17), NMO (n = 23), and MS (n = 25) who had brain stem lesions on MRI were enrolled. Morphological features of brain stem lesions among these diseases were assessed.
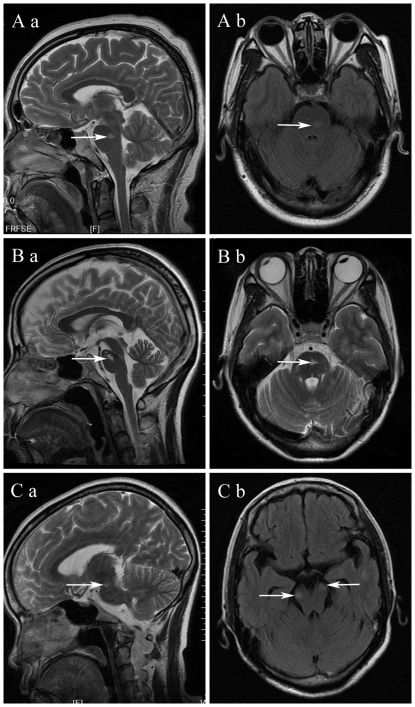
Results: Patients with ADEM had a higher frequency of midbrain lesions than did patients with NMO (94.1% vs. 17.4%, P<0.001) and MS (94.1% vs. 40.0%, P<0.001); patients with NMO had a lower frequency of pons lesions than did patients with MS (34.8% vs. 84.0%, P<0.001) and ADEM (34.8% vs. 70.6%, P = 0.025); and patients with NMO had a higher frequency of medulla oblongata lesions than did patients with ADEM (91.3% vs. 35.3%, P<0.001) and MS (91.3% vs. 36.0%, P<0.001). On the axial section of the brain stem, the majority (82.4%) of patients with ADEM showed lesions on the ventral part; the brain stem lesions in patients with NMO were typically located in the dorsal part (91.3%); and lesions in patients with MS were found in both the ventral (44.0%) and dorsal (56.0%) parts. The lesions in patients with ADEM (100%) and NMO (91.3%) had poorly defined margins, while lesions of patients with MS (76.0%) had well defined margins. Brain stem lesions in patients with ADEM were usually bilateral and symmetrical (82.4%), while lesions in patients with NMO (87.0%) and MS (92.0%) were asymmetrical or unilateral.
Conclusions: Brain stem lesions showed various morphological features among adult patients with ADEM, NMO, and MS. The different lesion locations may be helpful in distinguishing these diseases.
Conflict of interest statement
Figures


References
-
- Brinar VV. Non-MS recurrent demyelinating diseases. Clin Neurol Neurosurg. 2004;106:197–210. - PubMed
-
- Charil A, Yousry TA, Rovaris M, Barkhof F, De Stefano N, et al. MRI and the diagnosis of multiple sclerosis: expanding the concept of “no better explanation”. Lancet Neurol. 2006;5:841–852. - PubMed
-
- Fukazawa T, Kikuchi S, Niino M, Yabe I, Miyagishi R, et al. Attack-related severity: a key factor in understanding the spectrum of idiopathic inflammatory demyelinating disorders. J Neurol Sci. 2004;225:71–78. - PubMed
-
- Poser S, Luer W, Bruhn H, Frahm J, Bruck Y, et al. Acute demyelinating disease. Classification and non-invasive diagnosis. Acta Neurol Scand. 1992;86:579–585. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
