

Elevated hemostasis markers after pneumonia increases one-year risk of all-cause and cardiovascular deaths
- PMID: 21853050
- PMCID: PMC3154260
- DOI: 10.1371/journal.pone.0022847
Elevated hemostasis markers after pneumonia increases one-year risk of all-cause and cardiovascular deaths
Abstract
Background: Acceleration of chronic diseases, particularly cardiovascular disease, may increase long-term mortality after community-acquired pneumonia (CAP), but underlying mechanisms are unknown. Persistence of the prothrombotic state that occurs during an acute infection may increase risk of subsequent atherothrombosis in patients with pre-existing cardiovascular disease and increase subsequent risk of death. We hypothesized that circulating hemostasis markers activated during CAP persist at hospital discharge, when patients appear to have recovered clinically, and are associated with higher mortality, particularly due to cardiovascular causes.
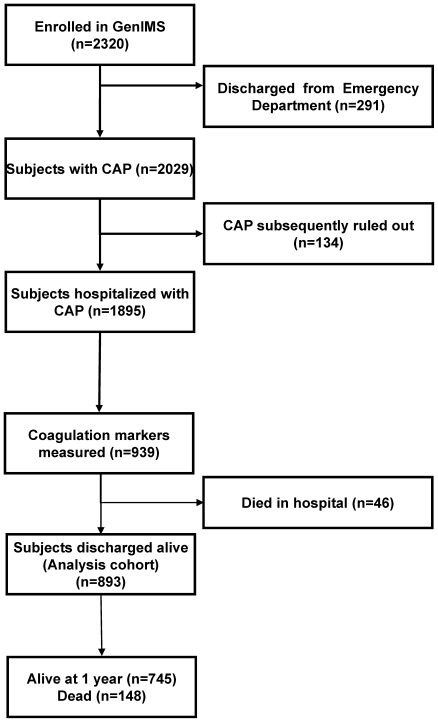
Methods: In a cohort of survivors of CAP hospitalization from 28 US sites, we measured D-Dimer, thrombin-antithrombin complexes [TAT], Factor IX, antithrombin, and plasminogen activator inhibitor-1 at hospital discharge, and determined 1-year all-cause and cardiovascular mortality.
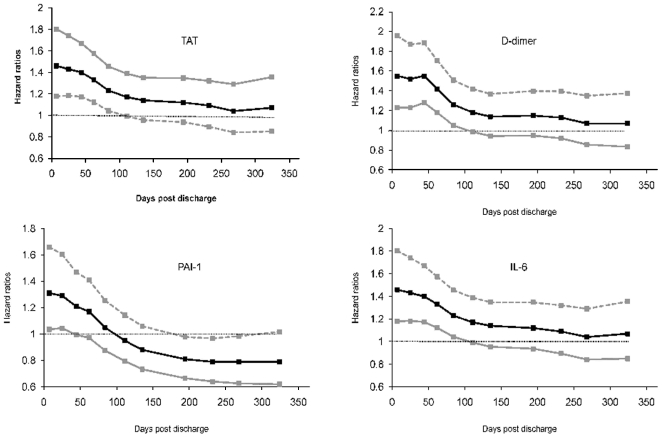
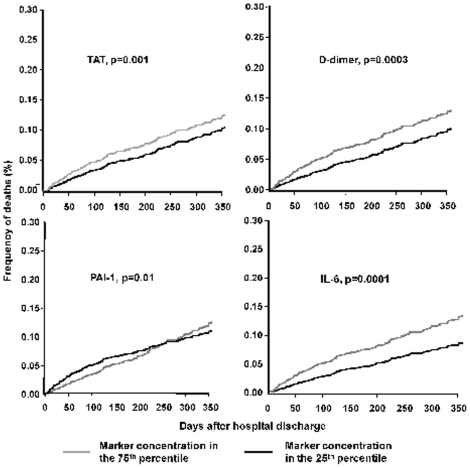
Results: Of 893 subjects, most did not have severe pneumonia (70.6% never developed severe sepsis) and only 13.4% required intensive care unit admission. At discharge, 88.4% of subjects had normal vital signs and appeared to have clinically recovered. D-dimer and TAT levels were elevated at discharge in 78.8% and 30.1% of all subjects, and in 51.3% and 25.3% of those without severe sepsis. Higher D-dimer and TAT levels were associated with higher risk of all-cause mortality (range of hazard ratios were 1.66-1.17, p = 0.0001 and 1.46-1.04, p = 0.001 after adjusting for demographics and comorbid illnesses) and cardiovascular mortality (p = 0.009 and 0.003 in competing risk analyses).
Conclusions: Elevations of TAT and D-dimer levels are common at hospital discharge in patients who appeared to have recovered clinically from pneumonia and are associated with higher risk of subsequent deaths, particularly due to cardiovascular disease.
Conflict of interest statement
Figures
References
-
- Brancati FL, Chow JW, Wagener MM, Vacarello SJ, Yu VL. Is pneumonia really the old man's friend? Two-year prognosis after community-acquired pneumonia. Lancet. 1993;342:30–33. - PubMed
-
- Kaplan V, Clermont G, Griffin MF, Kasal J, Watson RS, et al. Pneumonia: still the old man's friend? Arch Intern Med. 2003;163:317–323. - PubMed
-
- Koivula I, Sten M, Makela PH. Prognosis after community-acquired pneumonia in the elderly: a population-based 12-year follow-up study. Arch Intern Med. 1999;159:1550–1555. - PubMed
-
- Waterer GW, Kessler LA, Wunderink RG. Medium-term survival after hospitalization with community-acquired pneumonia. Am J Respir Crit Care Med. 2004;169:910–914. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
