

Clinical sensitivity and specificity of multiple T2-hyperintensities on brain magnetic resonance imaging in diagnosis of neurofibromatosis type 1 in children: diagnostic accuracy study
- PMID: 21853543
- PMCID: PMC3160695
- DOI: 10.3325/cmj.2011.52.488
Clinical sensitivity and specificity of multiple T2-hyperintensities on brain magnetic resonance imaging in diagnosis of neurofibromatosis type 1 in children: diagnostic accuracy study
Abstract
Aim: To determine the prevalence, number, and location of multiple (≥2) T2-hyperintensities on brain magnetic resonance imaging (MRI) in children with neurofibromatosis type 1 (NF1) and their correlation with age, and to establish their sensitivity, specificity, and accuracy for the diagnosis of NF1 in children, especially in the early age (2-7 years).
Methods: We performed a cross-sectional study of 162 patients with NF1 from Croatian Neurofibromatosis Association Database and 163 control children between the ages of 2 and 18 years who underwent brain MRI between 1989 and 2009.
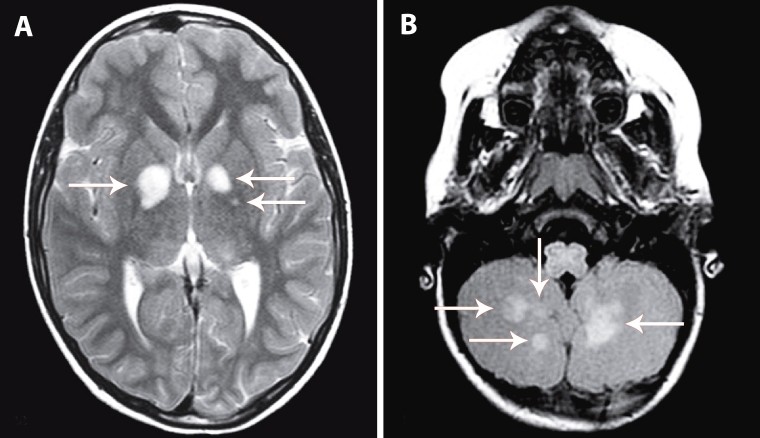
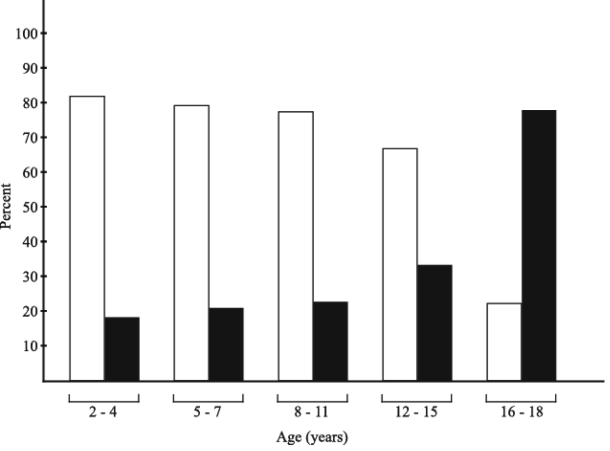
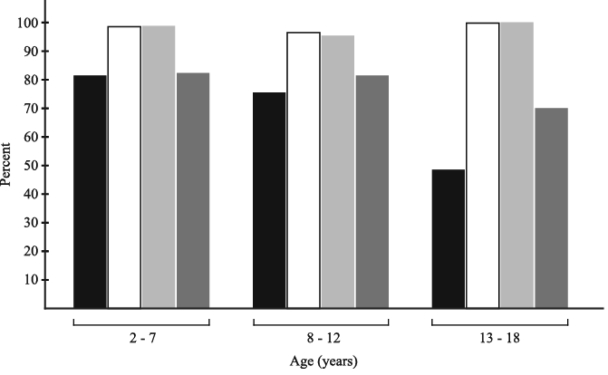
Results: Multiple T2-hyperintensities were present in 74% of NF1 patients and 1.8% of controls. They were mainly located in the basal ganglia, brainstem, and cerebellum and were significantly decreased in prevalence and number in the older age. T2-hyperintensities had excellent diagnostic accuracy with the area under the receiver operating characteristic (ROC) curve of 0.849 and 95% confidence interval (CI) of 0.805-0.886. The diagnostic sensitivity, specificity, and accuracy rate of T2-hyperintensities for NF1 were highest in the youngest age (2-7 years): 81% (95% CI 71%-89.1%), 99% (95% CI 92.3%-100%), and 85.8 (95% CI 83.3-93.8), respectively.
Conclusion: This study strongly suggests the inclusion of T2-hyperintensities on brain MRI on the list of diagnostic criteria for NF1, especially in children of early age, when the clinical penetration of the NF1 gene has not yet been completely finished.
Figures


References
-
- Crowe FW, Schull WJ, Neel JV. A clinical, pathological, and genetic study of multiple neurofibromatosis. Springfield, (IL): Charles C. Thomas; 1956.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous